By: Samantha R. Saravana-Bawan, MD, FRCP Karen Letourneau, CRGS
Clinical Images
Ultrasonographic findings and treatment in heterotopic cesarean scar pregnancy
Issue: BCMJ,
vol. 66, No. 6, July August 2024,
Pages 202-203 Clinical Articles Clinical Images
A very rare case of heterotopic cesarean scar pregnancy highlights the potential for cesarean scar pregnancy in patients with a history of cesarean scar.
History
A pregnant woman in her mid-30s presented to the emergency room with acute onset of back and pelvic pain and moderate spotting. The patient was gravida 4, para 2 (G4P2) and had had two prior cesarean sections. The pregnancy was conceived using letrozole as a fertility medication, which has a known twin risk of 3% to 7%.[1] Estimated gestational age was 5 weeks 3 days. Quantitative β-hCG level was 7190 mIU/mL at presentation and rose to 13 484 mIU/ mL 2 days later.
Imaging findings
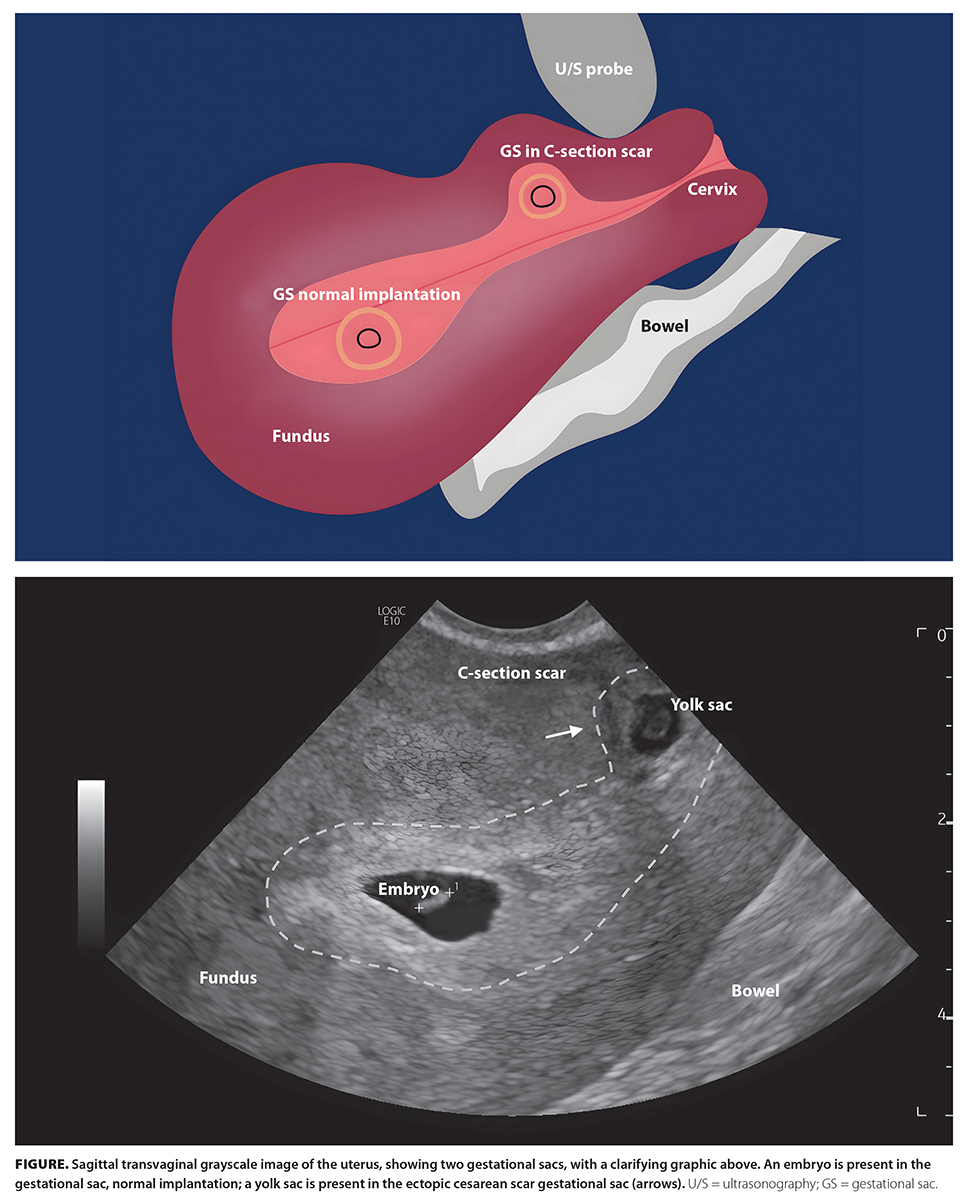
Ultrasonography showed a gestational sac with an embryo implanted in the endometrium near the fundus and an ectopic gestational sac within the cesarean scar niche [Figure].
Discussion
Imaging findings of two gestational sacs, where one sac is implanted along the cesarean scar, suggests heterotopic cesarean scar pregnancy. The patient wished to keep the intrauterine gestation; thus, a selective reduction of the cesarean scar pregnancy by ultrasonography-guided local injection of methotrexate was performed. Despite this, the patient’s β-hCG level continued to rise. Systemic treatment with methotrexate also failed to reduce the β-hCG level; therefore, a hysterectomy was performed. Heterotopic cesarean scar pregnancy was confirmed at pathology.
Heterotopic pregnancy is one of the rarest forms of multiple gestation, occurring in less than 1 in 30 000 naturally conceived pregnancies.[2] The incidence of heterotopic pregnancy increases with assisted reproductive techniques.[3] Cesarean scar pregnancy is extremely rare and accounts for only 6% of all ectopic pregnancies; however, incidences are rising with cesarean section rates.[4] Heterotopic cesarean scar pregnancy is a rare cesarean scar pregnancy combined with an intrauterine pregnancy.
Treatment for isolated cesarean scar pregnancy includes dilation and curettage, laparoscopic resection, and local or systemic administration of methotrexate.[5] Because of the low incidence of heterotopic cesarean scar pregnancy, no standard treatment protocols have been established.
Ultrasonography-guided selective embryo aspiration and/or drug injection and surgical resection have been described.[6]
Competing interests
None declared.
hidden
This article has been peer reviewed.
 |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. |
References
1. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. N Engl J Med 2014;371:119-129. Erratum in: N Engl J Med 2014;317:1465.
2. Hassani KIM, El Bouazzaoui A, Khatouf M, Mazaz K. Heterotopic pregnancy: A diagnosis we should suspect more often. J Emerg Trauma Shock 2010;3:304.
3. Abusheikha N, Salha O, Brinsden P. Extra-uterine pregnancy following assisted conception treatment. Hum Reprod Update 2000:6:80-92.
4. Singh K, Soni A, Rana S. Ruptured ectopic pregnancy in caesarean section scar: A case report. Case Rep Obstet Gynecol 2012;2012:106892.
5. Karahasanoglu A, Uzun I, Deregözü A, Ozdemir M. Successful treatment of cesarean scar pregnancy with suction curettage: Our experiences in early pregnancy. Ochsner J 2018;18:222-225.
6. OuYang Z, Yin Q, Xu Y, et al. Heterotopic cesarean scar pregnancy: Diagnosis, treatment, and prognosis. J Ultrasound Med 2014;33:1533-1537.
hidden
Dr Saravana-Bawan is an interventional radiologist in the Island Health Authority. Ms Letourneau is a sonographer in the Island Health Authority.
Corresponding author: Karen Letourneau, karenletourneau@me.com.
