Streptococcus pyogenes is alive and well
Issue: BCMJ,
vol. 51 , No. 3 , April 2009 ,
Pages 122-127 Clinical Articles
A recent case with the uncommon citation of acute rheumatic fever must remind physicians of the ever-present burden of Streptococcus pyogenes infections. Although largely represented in episodes of strep throat, postinfectious sequelae continue to attract attention, most recently with the addition of pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). The occurrence of severe S. pyogenes infections is cyclical and in accord with the community frequency of strep throats. Treatment aspects have been complicated by the rising incidence of macrolide and clindamycin resistance, although penicillin and other beta-lactam agents continue to demonstrate strong in vitro activity. Several aspects of diagnosis are challenging. Rapid diagnostic tests have a number of limitations. As well, nonhemolytic and non-group A streptococci can be the cause of infection and should be considered. With the prospect of a vaccine still far away, S. pyogenes will remain alive and well.
Fortunately, S. pyogenes continues to be susceptible to penicillin and other beta-lactam agents.
In the minds of family physicians, Streptococcus pyogenes has historically been associated primarily with strep throat and, secondarily, with the complications of rheumatic fever and glomerulonephritis. The latter complications have largely diminished in the antibiotic era. Despite such a reduction in complications, infection due to S. pyogenes has continued to attract considerable attention for various reasons. In the last 2 decades, for example, the entities of streptococcal toxic shock and invasive S. pyogenes infections have provided renewed interests. A recent case illustrates how S. pyogenes-associated acute rheumatic fever and nephritis continue to be seen.
A 20-year-old man presented to a medical clinic in the summer of 2008 with body aches, generalized stiffness, swollen hands and feet, and mild pharyngeal irritation with cough. He had experienced a mild upper respiratory tract infection some 2 weeks before, but did not seek medical attention at that time because of a busy work schedule.
The patient was afebrile, and on examination his body aches appeared to be confined to the joints of all limbs. Although the hands were generally swollen, the changes were most evident at the phalangeal and metacarpal-phalangeal joints. He had evidence of bilateral mild conjunctival injection, but there was no peripheral rash. The oropharynx was mildly inflamed, and the tonsils and anterior cervical lymph nodes were modestly prominent. No heart murmur or neurological signs were detected. A throat swab was taken, and the patient was referred to the laboratory for further investigations. He was advised to consume ibuprofen on an as-needed basis.
The throat swab yielded group A streptococcus. The peripheral white blood cell count was 8.2 with a normal differential. Test results for acute mononucleosis and acute parvovirus infection were negative, and assays for liver function, antinuclear antibody, and rheumatoid factor were unremarkable. Microscopic urinalysis showed the presence of hematuria, and the quantitative urinary protein was 5 g/L. The creatinine level was 112 µmol/L, and the estimated glomerular filtration rate was 67 mL/min/1.73 m2. An electrocardiogram showed sinus rhythm of 77/min, with first-degree AV block and ST elevation in the anterolateral leads. The antistreptolysin O titer was 217 IU/mL.
A course of penicillin V (300 mg q.i.d. for 10 days) was begun. After 2 weeks, the patient was completely well. Both microscopic hematuria and proteinuria were no longer apparent, and the antistreptolysin O titer increased to 230 IU/mL. The patient has since remained well.
Acute rheumatic fever
In the case described here, the latent period of approximately 2 weeks between respiratory illness and subsequent manifestations of acute rheumatic fever is typical. The gap is a consequence of the delayed immunological response to the S. pyogenes bacterium, in which cross-reactive host antigens are also targeted.[1] This patient suffered from arthropathy and carditis and had supporting laboratory studies. However, this rare citation of acute rheumatic fever is difficult to place in context because acute rheumatic fever is not a reportable communicable disease in BC[2] and there is no mandate to report acute rheumatic fever Canada-wide.[3] Outbreaks and endemic prevalence in Canada have been reported, however, from Nova Scotia and Manitoba over the last few decades.
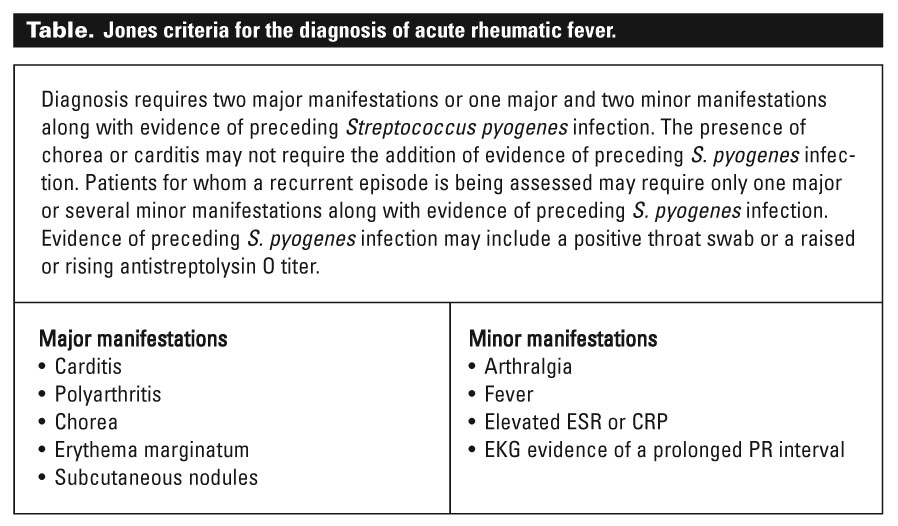
Given the variability in clinical presentation and the lack of an absolute single and infallible diagnostic test for acute rheumatic fever, the Jones criteria (Table) were established to accurately diagnose infection and minimize the potential overdiagnosis that could result if more generalized and less specific clinical criteria were used. As with many other illnesses that are diagnosed using predominantly clinical criteria, however, variations from the classical definitions are likely to arise over time. For example, poststreptococcal reactive arthritis does not fulfill the Jones criteria, but nevertheless shares a number of features with acute rheumatic fever.[4] A nonpyogenic arthropathy with a slightly shorter latency period than acute rheumatic fever, poststreptococcal reactive arthritis can affect both large and small joints but is usually nonmigratory. Some patients experience an associated carditis. The similarities to the postinfectious immune events of acute rheumatic fever have prompted some experts to advocate antistreptococcal prophylaxis.[4] Poststreptococcal reactive arthritis could therefore be considered an addendum to the variations of acute rheumatic fever.
Another example of similar phenomena was reported by Munn and colleagues at BC’s Children’s Hospital, where a child was found to have acute encephalomyelitis as a late poststreptococcal neurological manifestation.[5] The authors argued for extending the neurological spectrum of acute rheumatic fever (formerly regarded as consisting mainly of Sydenham’s chorea), which has since been supported by other reports worldwide.
Enter PANDAS
Some 10 years ago, the pediatric community was presented with a new hypothesis for the origin of childhood tics and obsessive-compulsive disorders.[6] It was proposed that such conditions were due to a poststreptococcal immune response termed pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS), which produces antibodies that cross-react with the basal ganglia of the brain, thus again theoretically expanding on the neurological manifestations of acute rheumatic fever. PANDAS has provoked much controversy among generalists, pediatric neurologists, and psychiatrists. Gabbay and colleagues recently demonstrated how such an entity can quickly gain medical and public attention, and how the latter can translate into unwarranted diagnosis and treatment.[7] Others have warned the medical community previously to exercise caution when considering PANDAS.[6] The PANDAS entity, if valid, may be critical to understanding poststreptococcal immune events.
Toxic shock and invasive infections
Although severe S. pyogenes invasive infections have been recognized for as long as the bacterium has been known, there appeared to be an increase in such infections in the late 1980s in North America. Some of these illnesses included a progression to multiorgan failure and cardiovascular shock. Others included the finding of invasive group A streptococci in usually sterile sites, and yet others included aggressive soft tissue infections such as necrotizing fasciitis. It is recognized that S. pyogenes can exist in many different types, which largely vary in their surface antigenic (M and T protein) makeup. In the 1980s, a few such types appeared to increase in prevalence worldwide, and it was postulated that the use of antibiotics may have led to a reduction in natural immunity at a time when some of the types were gaining a stronghold.
In British Columbia, the increase in such aggressive infections was paralleled by an increase in scarlet fever and strep throat diagnoses.[8] A majority of the invasive infections were due to the M1T1 type, a situation found in many other parts of the world experiencing such resurgence. Recent data for this province suggest an apparent tripling of reportable invasive infections from 1998 to 2006.[9] While the bacterium remains susceptible to penicillin, the co-administration of clindamycin may be beneficial when necrotizing fasciitis is a concern. Some have recommended the use of intravenous immune globulin as well. The dramatic nature of these infections has prompted some to advocate antibiotic prophylaxis for family contacts, an approach considered unnecessary by others.[10]
Antibiotic susceptibility and resistance
Given the plethora of bacteria that have demonstrated problematic antibiotic resistance since the beginning of the antibiotic era, the continuing susceptibility of S. pyogenes to penicillin and other beta-lactam antibiotics is a natural wonder. It is especially surprising that penicillin resistance has not been found by conventional laboratory methods when we know that this bacterium can be a component of the usual oropharyngeal bacterial flora and hence considerably exposed to the effects of both orally and parenterally administered antibiotics, most of which have historically been beta-lactam agents. Penicillin and first-generation cephalosporins are still highly active against S. pyogenes as are variations of the same in the form of new cephalosporins.
Although beta-lactam agents are mainly used to treat S. pyogenes infections, alternatives must be utilized for penicillin-allergic patients. Sulphonamides and tetracycline are not recommended as alternatives for strep throat. Instead, alternatives commonly include erythromycin, clarithromycin, and azithromycin. Clindamycin may be employed to treat problematic carriers or some invasive infections. For most isolates, macrolide resistance and clindamycin resistance are linked genetically. Historically, mac-rolide resistance was very low. For instance, at BC’s Children’s Hospital, we determined the frequency of such resistance to be less than 3% in the early 1990s. Worldwide, however, macrolide and clindamycin resistances have materialized, with reports of resistance between 10% and 40%. Locally, such resistance has also been documented by two large private laboratories: LifeLabs[11] published erythromycin and clindamycin resistance rates of 44% and 42%, respectively, from their Burnaby and Victoria laboratories in 2005, while BC Biomedical[12] found rates of 15% resistance at their Lower Mainland laboratories in 2007. This change has been attributed to the increased use of clarithromycin and azithromycin for respiratory infections, especially in pediatrics. As the use of macrolides in pediatrics continues to enjoy a resurgence alongside a reduction in the use of new cephalosporins, such instances of resistance are likely to continue and may increase. Clinicians need to indicate on their laboratory requisitions for throat swabs whether the patient is to commence a macrolide or clindamycin treatment or if the patient is known to have a penicillin allergy so that the microbiology laboratory can specifically determine such resistance for the isolates of S. pyogenes in a context where it is not routinely performed.
Treatment of primary streptococcal pharyngitis
The historic use of benzathine penicillin injections for the treatment of streptococcal pharyngitis is largely not ascribed to now, and oral penicillin V for 10 days has been the contemporary standard for decades. For most patients, this standard treatment is sufficient. First-generation cephalosporins were found to be efficacious for strep throat after they were first widely introduced, and macrolides proved to be effective for penicillin-allergic patients. Newer macrolides and cephalosporins have also been used and popularized by some.
Various aspects of strep throat treatment have received attention in a large number of clinical trials. Some have shown that short courses of penicillin treatment are inferior to the standard 10-day course for both short-term clinical and bacteriological cure rates.[13] Some trials have shown that short courses of cephalosporin therapy can be equal to or better than penicillin V, and that short courses of macrolides are not better than 10 days of penicillin V.[13] Whether for cephalosporins as a group or for individual cephalosporins, outcomes of their use have generally been equal or superior to penicillin. Unfortunately, the sizes of studies that have demonstrated comparable efficacy have not been large enough to determine differences in the outcome of subsequent acute rheumatic fever or other postinfectious sequelae.
Newer macrolides and cephalosporins are significantly more expensive than penicillin V. Most of these agents also have a considerably broader antimicrobial spectrum than penicillin V, and hence raise concerns about inducing resistance. Likewise, the common use of amoxicillin in place of penicillin V, while beneficial for some in terms of palatability or absorption, raises the same concerns because amoxicillin too has a significantly greater spectrum of antimicrobial activity than penicillin V. It is not surprising that authors of contemporary research papers continue to advocate a 10-day course of penicillin V.[14]
Recurrent pharyngitis and oropharyngeal carriage
Many reasons have been proposed to account for the failure of antibiotic treatment. Factors in treatment failure can be viewed as short-term clinical, long-term clinical, or bacteriological. Some patients will have an early relapse measured in days or weeks after completing treatment. Such relapsing infection often involves the same strain of S. pyogenes and on occasion takes the form of up to three relapses. Other patients have recurrent sore throat over many months, and the infection may involve the same strain or different newly acquired strains. Patients who do not respond to initial therapy can be treated again with amoxicillin, a cephalosporin, clindamycin, or a beta-lactam agent with the addition of rifampin. Bacteriological failure refers to the ability to find S. pyogenes on repeat throat swabs after a full course of appropriate antibiotic and despite a clinical cure. There are few circumstances when such follow-up cultures are warranted, and, in general, posttreatment throat swabs are not recommended given that some patients will become asymptomatic carriers.
Antibiotic treatment failure is commonly related to poor compliance with a 10-day regimen. Other factors may include exposure to a new strain, poor immune response as a consequence of early antibiotic administration, diminished antibiotic penetration into tonsillar crypts, and protective effects of other nearby oropharyngeal flora. Some treated patients may actually have been carriers all along.
S. pyogenes carriage in the oropharynx may vary from 3% to 15%, the frequency of which will depend on the endemicity of acute infections. Given this frequency, however, it is likely that approximately one in every 10 to 20 throat swabs will yield the bacterium, even though the patient is truly infected by a virus. If throat swabs are obtained mainly from patients who are not clinically typical for having strep throat, and given that the incidence of strep throat may be only about 20% to 50% in these patients, it is conceivable that 1 in every 5 to 10 positive throat swabs are falsely indicative of acute infection. Use of the antistreptolysin O titer serology may be relevant to diagnosis, therefore, in postinfectious complications of S. pyogenes respiratory infection. The number of S. pyogenes bacteria in a throat swab compared with the usual oropharyngeal bacteria is low, but laboratories unfortunately often report only the presence or absence of group A streptococci rather than their presence semi-quantitatively compared with normal flora for the same specimen.[15] The provision of such information would be welcome.
Rapid diagnostic tests
The need to avoid delays in obtaining throat swab microbiology results and to improve on the clinical utility of diagnosis has prompted the development of rapid diagnostic tests for strep throat. Such tests are analogous to those used for rapid diagnosis of pregnancy in office settings. The implementation of these tests for S. pyogenes in primary care was assessed extensively in the mid-1980s by the family practice research group at the University of Calgary,[16] who found a number of logistical complexities despite what was a seemingly simple assay.[17]
Whereas specimen acquisition and initial processing steps are rather easy to accomplish, the acumen of individuals performing such an assay is still critical. In primary care, the tests are usually performed by medical office assistants, whose expertise in the nuances of such assays are limited. The frequency of false-negative assays necessitated that such negative rapid tests would require follow-up with a routine microbiology culture. The latter could be required for up to 70% of specimens or more.
The potential for both false-positive and false-negative results has led to some trepidation in adopting these assays. There is also concern that rapid tests will not detect non-group A pharyngeal pathogens or give information on macrolide resistance, which is becoming more prevalent. Finally, primary care physicians in British Columbia are not compensated for using such rapid diagnostic test kits, and it is perhaps this disincentive that has most affected poor utilization rates of these tests in BC.
Nonhemolytic S. pyogenes
The traditional laboratory detection method for strep throat involves growth of bacteria from throat swabs on a bacteriological medium that highlights beta-hemolysis; that is, a clear halo appearance around a colony of the bacterium due to red blood cell degradation. Although this approach is still used today, it is not infallible. Nonhemolytic S. pyogenes do occur, albeit uncommonly. A report from BC’s Children’s Hospital published in 2002 illustrates the potential difficulties encountered when such a variant strain of S. pyogenes causes infection.[18] In this case 0.5% of throat swabs were found to contain such variant strains from generally submitted specimens. Given that strep throat is usually identified in approximately 10% to 30% of throat swabs submitted for diagnostic purposes in acute settings, this could translate into approximately 3% to 5% of strep throats being missed only because of a technological anomaly.
Non-group A streptococcal pharyngitides
Although S. pyogenes is the principal and time-honored cause of strep throat, the microbiological identification process of screening for beta-hemolytic streptococci has led many to wonder if other non-group A streptococci could cause sore throats or even postinfectious sequelae.[19] Not all group A streptococci are S. pyogenes, and other non-group A streptococci include many other Lancefield groups.
Physicians in British Columbia receive occasional reports of throat swabs with beta-hemolytic group C and group G streptococci, some subsets of which are thought to cause acute sore throats.[20] Unfortunately, many laboratories are not differentiating between potentially pathogenic and nonpathogenic group C and group G streptococci from throat swabs, and hence there is confusion when such a report is received. In common community-acquired pharyngitis, it is recommended that reports of group C and group G streptococci in throat swabs be considered for treatment if the patient continues to have sore throat symptoms.
Vaccination and future prospects
Although vaccination strategies continue to receive attention, no effective vaccine is available yet. The potential for a vaccine to induce a poststreptococcal-like immune response is high on the minds of those who study in this area, given the cross-reactivity of S. pyogenes and some human tissue. Experimental vaccines have taken into consideration the portions of antigenic but not cross-reactive areas of some M proteins. Although most infections in humans are caused by strains that have particular outer (M) proteins, there are many variations on the theme of such proteins. Vaccines will therefore need to include several of such M protein types, in the same way that several capsular types are included for pneumococcal vaccines. Even if a safe and protective vaccine is developed, there will continue to be concern about the emergence of lesser common M types in disease, again analogous to the emergence of lesser common pneumococcal serotypes in some regions where the multivalent pneumococcal vaccines have been introduced widely for pediatric use.
The ubiquity of S. pyogenes in the general population and the lack of natural protective immunity on a population basis will ensure that this pathogen continues to prevail. The frequency of invasive and devastating infections will parallel the frequency of strep throat in the general population. Even though we live in an antibiotic era, we will continue to experience acute rheumatic fever. And although the absence of penicillin-resistant S. pyogenes is extremely beneficial, the rising incidence of macrolide and clindamycin resistance will surely complicate some illnesses. Ongoing determinations of resistance would be prudent. Public health surveillance for poststreptococcal complications such as acute rheumatic fever are just as relevant now as they ever were, given the continuing challenges posed by S. pyogenes.
Competing interests
None declared.
References
1. Carapetis JR, McDonald M, Wilson NJ. Acute rheumatic fever. Lancet 2005;366:155-168.
2. British Columbia Centre for Disease Control. List of reportable communicable diseases in BC April 2008. www.bccdc.org/content.php?item=7 (accessed 11 February 2009).
3. Canadian Pediatric Society. Surveillance: Acute rheumatic fever. www.cps.ca/English/Surveillance/CPSP/Studies/rheumatic_fever.htm (accessed 11 February 2009).
4. Shulman ST, Ayoub EM. Poststreptococcal reactive arthritis. Curr Opin Rheumatol 2002;14:562-565.
5. Munn R, Farrell K, Cimolai N. Acute encephalomyelitis: Extending the neurological manifestations of acute rheumatic fever? Neuropediatrics 1992;23:196-198.
6. Kurlan R, Kaplan EL. The pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) etiology for tics and obsessive-compulsive symptoms: Hypothesis or entity? Practical considerations for the clinician. Pediatrics 2004;113:883-886.
7. Gabbay V, Coffey BJ, Babb JS, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcus: Comparison of diagnosis and treatment in the community and at a specialty clinic. Pediatrics 2008;122:273-278.
8. Cimolai N, Trombley C, Adderley RJ, et al. Invasive Streptococcus pyogenes infections in children. Can J Public Health 1992;83:230-233.
9. BC Centre for Disease Control. 2006 Epidemiology Report: Annual summary of Reportable Diseases. Vancouver: BCCDC; 2007:46. www.bccdc.org/downloads/pdf/epid/reports/Epid-annual-06-Final.pdf (accessed 11 February 2009).
10. Smith A, Larmagni TL, Oliver I, et al. Invasive group A streptococcal disease: Should close contacts routinely receive antibiotic prophylaxis? Lancet Infect Dis 2005;5:494-500.
11. LifeLabs. Antimicrobial susceptibility profile. 2005. www.mdsdx.com/Lifelabs_BC/Health_Care/Antimicrobial_Susceptibility_Profi... (accessed 11 February 2009).
12. BC Biomedical Laboratories. Empiric therapy antibiogram 2007. Physicians’ Newsletter 2008;10(1):2. www.bcbio.com/uploadedFiles/Physicians/Physician’s_Newsletter/newsletters/Volume 10, Issue 1–Final for Web–Aug 21 2008.pdf (accessed 11 February 2009).
13. Casey JR, Pichichero ME. Metaanalysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Pediatr Infect Dis J 2005;24:909-917.
14. Falagas ME, Vouloumanou EK, Matthaiou DK, et al. Effectiveness and safety of short-course vs long-course antibiotic therapy for group A beta hemolytic streptococcal tonsillopharyngitis: A meta-analysis of randomized trials. Mayo Clin Proc 2008;83:880-889.
15. Anand C, Cimolai N. Critical features of specimen collection, transport, and processing. In: Cimolai N (ed). Laboratory Diagnosis of Bacterial Infections. New York: Marcel Dekker; 2001.
16. Elford RW, Cimolai N, Anand CM, et al. The impact of a rapid streptococcal diagnostic kit on the management of primary care patients. Presented at XVI World Congress of Anatomic and Clinical Pathology, Vancouver, BC, 1991.
17. Cimolai N. Detection of streptococcal antigens: Arguments for and against testing in primary care offices. Clin Biochem 1993;26:27-29.
18. Cimolai N, Trombley C, Bhanji NM. Nonhemolytic Streptococcus pyogenes causing invasive infection. Clin Pediatr (Phila) 2002;41:453.
19. Cimolai N, Elford RW, Bryan L, et al. Do the beta-hemolytic non-group A streptococci cause pharyngitis? Rev Infect Dis 1988;10:587-601.
20. Cimolai N, Morrison BJ, MacCulloch L, et al. Beta-hemolytic non-group A streptococci and pharyngitis: A case-control study. Eur J Pediatr 1991;150:776-779.
Dr Cimolai is a medical microbiologist in the Program of Microbiology, Virology, and Infection Control at Children’s and Women’s Health Centre of British Columbia. He is also a professor in the Department of Pathology and Laboratory Medicine at the University of British Columbia.

{kind=link}