Distant thoracic surgical patient assessment in rural British Columbia 1985-2005
Issue: BCMJ,
vol. 48 , No. 6 , July August 2006 ,
Pages 279-284 Clinical Articles
Patient access to specialty care decreases in areas of low population density such as British Columbia’s Interior and North. In 1985, distant on-site thoracic surgical clinics were developed in response to the difficulty of providing specialty care outside Victoria, Vancouver, and the Lower Mainland. In 2003, with the advent of new technologies, distant patient assessment evolved to a telemedicine model. Two thousand thirty-five patients were seen during 107 on-site clinics, and between December 2003 and December 2005, 872 patients were seen during 115 telemedicine clinics. When the two ways of assessing patients were compared, telemedicine was found to permit a significant increase in frequency of access to rural sites and greater numbers of patients seen. Patient satisfaction with telemedicine was also found to be very high. Despite some limitations, telemedicine clinics are now preferred over on-site clinics for rural patient thoracic surgical assessment.
Distant thoracic surgical patient assessment in rural British Columbia: The evolution from on-site clinics to telemedicine clinics, 1985–2005
British Columbia, like many Canadian provinces, has areas of both high and low population density (oral communication, P. Blumel, cartographer, Province of BC, 22 September 2005). People living in the expanse of BC beyond the well-populated southwest region have historically had more difficulty accessing specialty and subspecialty medical care.[1,2]
One million people live within the jurisdictions of the Interior Health Authority (IHA) and Northern Health Authority (NHA). The population density for this combined zone is 1.2 persons per square kilometre, substantially lower than the Canadian national average of 3.2 persons per square kilometre (see Table 1). This presents a particular challenge to thoracic patient surgical assessment.
Thoracic surgeons form the smallest adult surgical specialty group. The Canadian Association of Thoracic Surgeons has recommended standards of care for thoracic surgical practice.[3] To meet these standards and provide sustainability of practice, thoracic surgeons in BC have had to practise in groups delivering centralized surgical care. This reality was reinforced in British Columbia during the 1990s, when one thoracic surgeon entered practice while 10 full-time or part-time thoracic surgeons left practice.[4]
Thoracic surgery is primarily an oncology-focused subspecialty (lung, esophagus, and other). Patient assessment typically requires urgent but not emergent care. Investigations are usually complex due to associated comorbidities, most commonly cardiac and respiratory in nature. Patients typically proceed to major surgical procedures. Computerized tomography scanning is the main preassessment investigative tool, along with fine needle aspiration biopsy, pulmonary function assessment, and nuclear medicine evaluation.
Between 1985 and 2005, the way we assessed thoracic surgical patients in BC’s Interior and North evolved. First, we moved from relying on solo practitioners to using on-site clinics. Then, after December 2003, we began to use telemedicine with increasing frequency. In the Interior, the majority of patients undergoing distant assessment are now being seen using telemedicine techniques. In the North, many patients are now being assessed this way.
We believe that telemedicine is continuing to improve patient access, as well as reducing time to assessment and time to treatment. Keeping patients in their home communities as much as possible provides significant financial and social advantages to the patient and his or her family.
Development of on-site clinics
The first on-site outreach clinics were established when thoracic surgeons practising outside Victoria and the Lower Mainland began finding solo practice unsustainable. These surgeons were often doing additional work in general surgery or vascular surgery, as their communities required, and had to maintain constant availability. Furthermore, the international shortage of thoracic surgeons had made recruitment of new surgeons impossible.
The changing practice arrangements of the authors of this paper illustrate how thoracic surgical assessment has evolved since 1985.
Between 1985 and 1991, Vancouver-based Dr Bill Nelems (BN) conducted on-site consultation and follow-up clinics in Kelowna every 6 weeks. When Dr Andrew Luoma (AL) established a thoracic surgery practice in Kelowna in 1991, these outreach clinics were stopped.
From 1985 to 1991, BN and his two Vancouver-based partners, Drs Richard Finley and Ken Evans, ran on-site consulting and bronchoscopy clinics in Prince George. Before these clinics were operating, patients were required to travel 778 km to Vancouver for diagnostic bronchoscopy procedures.
From October 1995 until April 1998, Dr Michael Humer (MH) conducted a thoracic surgical practice in Prince George. In May 1998, he relocated his practice to Kamloops. While in Kamloops, MH also ran monthly on-site clinics in Prince George, and he continued to do so when he moved to Kelowna. For his Prince George clinics, MH was able to access the Northern and Isolation Travel Assistance Outreach Program (NITAOP) that compensated for travel expenses. With the advent of the assistance program, records were required and data remain available. Once in Kelowna, MH also began on-site clinics in Kamloops.
BN moved to practice in Kelowna in 1997. Between 1997 and 2002, BN provided monthly on-site clinics in Trail and Nelson in the West Kootenays. After 2002, BN also began on-site visits to Cranbrook in the East Kootenays. No NITAOP assistance was available for these clinics, and precise data for these clinics were not kept.
In December 2002, MH, AL, and BN came together to staff the IHA Kelowna site of the newly formed British Columbia Progamme of Thoracic Surgical Care, established by the Ministry of Health with the unanimous support of the BC Section of Chest Surgery.[5,6] The goal of this initiative was to provide quality thoracic surgical services to all British Columbians in a timely manner through centralized surgical units in Vancouver, Victoria, Surrey, and Kelowna. Three thoracic surgeons were assigned to each site and an alternative payment plan model was used.
While the on-site outreach clinics addressed the problems of solo practitioners, an increasing number of clinics were needed and these required increasing amounts of surgeon travel, raising the issues of sustainability and effective resource utilization, a common problem with other specialty outreach clinics in Canada.[7] Beginning in 2003, telemedicine clinics began to replace on-site clinics.
With IHA support, clinical and cost-impact studies were performed. Videoconferencing, previously used primarily for administrative purposes, was proposed as a way for physicians to provide distant care to patients.
Telemedicine clinics began in the East Kootenay region (Cranbrook) and the West Kootenay region (Trail and Nelson) in December 2003. They began in Kamloops in May 2004, in Prince George in July 2005, and in Williams Lake in October 2005.
Before the development of telemedicine, all new patient referrals were received in the Kelowna thoracic surgery home office. The home office triaged and coordinated all appointments, investigations, and surgical procedures. All patients with proven or suspected malignancy were triaged to be seen in consultation within 10 to 14 days of referral, either in Kelowna if the patient resided locally or by distant on-site assessment if they lived remotely.
At the on-site clinic, the thoracic surgeon met directly with patients and family members in the ambulatory care facilities of the local hospital. On-site secretarial or nursing assistance was not required.
With the advent of telemedicine for distant thoracic surgical assessment, the Interior and Northern Health authorities provided dedicated funding for each telemedicine site. This funding included both technical infrastructure and local clinical nurse support. The clinical nurses received ongoing local and Kelowna-based thoracic surgical education. The nurses accompanied the patients throughout the telemedicine process.
A dedicated clinical room for videoconferencing was set up at Kelowna General Hospital. Existing technology helped when linking this room with the other telemedicine sites. All acute care clinical sites within the IHA already had videoconferencing capacity via IP (Internet protocol), and all the health authorities in the province were already linked through a private network gateway (PNG).[8] Thus, sites within the IHA were already linked, and sites in the IHA and NHA could be linked by PNG for the secure exchange of health information.
Today, all distant clinical sites, including Prince George, have digital electronic radiology services (PACS or Picture Archive Communicating System),[9] making all radiological imaging from sites available to thoracic surgeons in Kelowna.
Within the IHA, a hospital-based electronic medical records system, Meditech Information Technology,[10] is used during the telemedicine assessment of Interior patients. More improvements concerning medical records are anticipated, with the NHA implementing a hospital-based electronic medical records system this year, and with the Kelowna thoracic surgery home office installing a paperless records system.[11]
All new distant patient consultations are now conducted by telemedicine. For patients with suspected thoracic malignancies, as many preoperative investigations as possible are performed at the distant sites. When indicated, these investigations include computerized tomography of the thorax and head, nuclear medicine bone scans, pulmonary function studies, fine needle biopsies, as well as routine hematology and serology. Except in Prince George and Kamloops, where diagnostic bronchoscopy services are available, all other diagnostic bronchoscopy studies are performed at the Kelowna General Hospital, usually in combination with staging mediastinoscopy procedures. All major surgical procedures are also performed in Kelowna. When patients arrive in Kelowna for their definitive surgery, specific components of the physical examination identified by the nurse at the telemedicine clinic or reported by the referring physician are verified. Patients with surgically unresectable disease are referred to the BC Cancer Agency and to supporting regional medical oncology units. Continued follow-up care is provided by telemedicine.
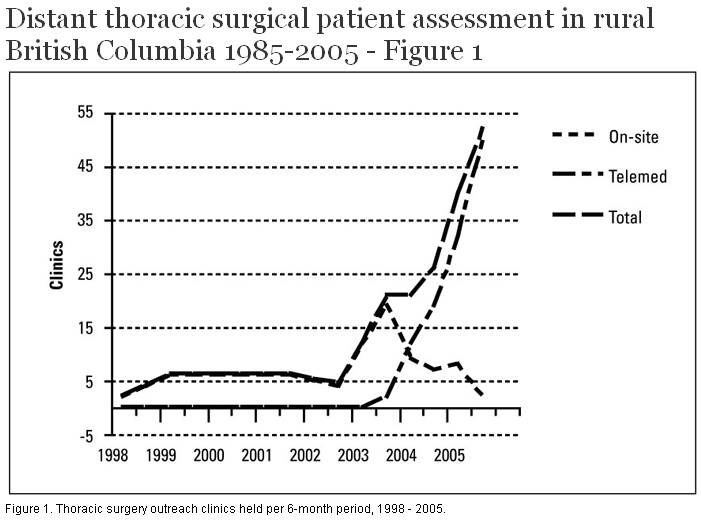
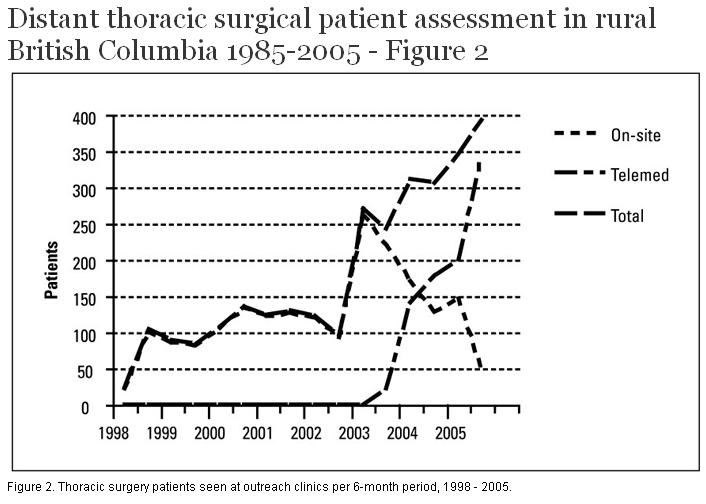
The introduction of telemedicine has allowed more patients to be assessed closer to where they live. Figure 1 shows the number of outreach clinics held every 6 months between June 1998 and December 2005, and how on-site clinics were eventually replaced by telemedicine clinics. Figure 2 shows how the number of outreach patients who were seen increased significantly after telemedicine clinics were introduced in December 2003.
{kind=link}
{kind=link}
In order to assess patient satisfaction with this change in service, patients visiting a telemedicine clinic in 2004 and 2005 were asked to complete a confidential questionnaire on their initial consultation and on their first follow-up visit. The questionnaire was completed by 273 new patients and 234 follow-up patients. Most patients were very satisfied with telemedicine services. Not only did patients find telemedicine “user friendly,” they also found the process saved them time and money. Both new and follow-up patients rated their satisfaction overall as 4.8 on a scale of 5 (see Table 2).
The high satisfaction ratings are not surprising given that we know patient access to specialist services is inversely related to the distance they live from major centres. The more remote the domicile, the less the patient accesses care.[2,12] Having specialists travel to conduct clinics in remote locations improves access to treatment,[12] and using telemedicine appears to improve access even more.
The development of on-site and telemedicine thoracic surgery clinics is by no means unique to BC. Researchers have considered the effect of having specialists travel to distant communities,[13,14] and described telemedicine services in a variety of remote locations.[15,16] BC’s story of thoracic surgery care to remote sites, however, is particularly timely and germane with the present convergence of specialist shortages, a history of on-site clinics, the advent of telemedicine technology, and the development of a provincial program with group practices. Arguably, northern and central British Columbia, with a very low population density of 1.2 persons per square kilometre, is an ideal testing ground for distant specialty services.
With the increasing number of telemedicine clinics (see Table 3), more patients are being seen more frequently (see Table 4). This was first noticed when the Kamloops outreach clinic converted from entirely on-site to entirely telemedicine clinics. When telemedicine became the standard mode of distant thoracic surgical patient assessment in Kamloops, more patients were seen and the time between clinics was reduced. This experience was replicated at all other distant sites when telemedicine replaced on-site clinics.
In terms of minimizing travel, telemedicine has helped both physicians and patients. For surgeons, the on-site clinics required more than 100 000 kilometres of travel for the time periods mentioned. For patients, the clinics required an estimated 2.5 million kilometres of travel. Eliminating much of this travel has meant significant savings in time, money, travel risk, and environmental impact.
The physical examination, which has an ingrained and almost ritualistic role in the assessment of the patient, is different at telemedicine clinics but still effective. A trained thoracic nurse attends the patient and provides invaluable support throughout the process. The nurse measures all vital signs, including oxygen saturation as required, and assists during the videoconference consultation. The visual inspection part of the physical examination remains intact. The physician can observe general medical status as well as facial expressions and demeanors. With the close-up camera view, the physician can examine postoperative wounds and look for visible physical features such as digital clubbing. Audiometric equipment allows for auscultation and permits the physician to hear heart sounds, breath sounds, bruits, and murmurs.[17] However, there is no equipment yet for palpation and percussion, and these aspects of the physical examination remain problematic with telemedicine.
As well as accompanying the patient during the videoconference process, many nurses act as useful local resource persons afterward. At some sites, the nurses that support the thoracic clinics also support the local chemotherapy units. For those patients returning for medical oncology treatments, the nurses offer further continuity of care.
While there are limitations to some parts of the physical examination with current telemedicine technology, telemedicine clinics are preferred to on-site clinics because they offer more frequent access and allow more patients to be seen over time. Patient compliance and satisfaction with the clinics are remarkably high. In addition, telemedicine is cost-effective for patients, surgeons, and health authorities, although true cost savings to both the patient and the health care system remain undetermined. Cost-impact analyses could clarify and inform future uses of this technology.
Physicians have an ethical responsibility to help reform and strengthen health care delivery.[18,19] By using telemedicine we can ensure that all patients with thoracic malignancies are seen within 2 weeks of referral, no matter how remote their residence. The principles of appropriate and timely access to specialty care can be met.
Future directions for telemedicine might include expansion of access to communities such as Terrace, Dawson Creek, Fort St. John, and Whitehorse. Other specialty services might use telemedicine to enhance distant patient access to care, and clinical researchers might use telemedicine technology to make connections with rural communities and their patients. As the use of telemedicine continues to evolve, specialists may one day be able to consult directly with patients in real time in the offices of their family doctors.
The authors wish to thank the Interior and Northern Health authorities, as well as K. Khoo, C. Mazurkewich, M. Loyola, A. Baldwin, L. Sawchenko, C. Markowski, R. Riley, J. McIntosh, S. Hardwicke, K. Whaley, R. Rochlin, D. Butcher, D. Horvat, H. Truran, C. Watkins, P. Baril, L. Blondin, V. Paolini, D. O’Brien, S. MacIntosh, L. Verigin, K. McLeod, V. Foster, D. Riel, L. Davidson, J. Ciancone, B. Mackay, K. Kin, L. Fehr, and D. Webb.
Competing interests
None declared.
Table 1. Population density: Canada, BC, and BC health authorities.
| Region | Population (million) | Area (km2) | Population density (persons per km2) |
| Canada | 32.10 | 9 970 610 | 3.2 |
| BC | 4.20 | 945 000 | 4.4 |
| Interior Health Authority | 0.70 | 215 495 | 3.3 |
| Fraser Health Authority | 1.44 | 15 665 | 92.0 |
| Vancouver Coastal Health Authority | 1.04 | 54 420 | 19.1 |
| Vancouver Island Health Authority | 0.71 | 55 040 | 12.9 |
| Northern Health Authority | 0.30 | 604 842 | 0.5 |
| Interior Health Authority and Northern Health Authority, combined | 1.00 | 820 337 | 1.2 |
Source: P. Blumel, cartographer, Province of BC.
Table 2. Patient satisfaction scores from telemedicine survey results.
| Question | New patient score* | First follow-up score |
| 1. Was your need for timely and appropriate consultation met? | 4.7 | 4.8 |
| 2. Did this process save you travel time and money? | 4.9 | 4.8 |
| 3. Did this process satisfy your need to meet and talk to the doctor? | 4.8 | 4.8 |
| 4. Did you receive adequate information regarding your medical condition? | 4.8 | 4.8 |
| 5. Was the videoconference process "user-friendly" (with the nurse on the one end and the doctor on the other)? | 4.8 | 4.9 |
| 6. Did you feel that every effort was made to respect your needs/thoughts/feelings? | 4.9 | 5.0 |
| Overall satisfaction (mean score for all questions) | 4.8 | 4.8 |
*Score: 1 (low) - 5 (high)
Table 3. On-site clinics for thoracic surgical assessment.
| Site | Dates operated | Clinics held | Consults completed | Follow-up visits | Patients seen | Clinics per 6-month period | Patients seen per clinic |
| Prince George | Jun 1998 -Jun 2005 | 76 | 416 | 1021 | 1437 | 5.4 | 18.9 |
| Kamloops | Feb 2003 - Mar 2004 | 12 | 108 | 191 | 299 | 5.1 | 24.9 |
| Cranbrook | Jun 2003 - Nov 2005 | 9 | 63 | 59 | 122 | 1.8 | 13.6 |
| Trail/Nelson | May 2000 - Nov 2005 | 10 | 80 | 97 | 177 | 2.0 | 17.7 |
| All sites | -- | 107 | 667 | 1368 | 2035 | n/a | 19.0 |
Table 4. Telemedicine clinics for thoracic surgical assessment.
| Site | Dates operated | Clinics held | Consults completed | Follow-up visits | Patients seen | Clinics per 6-month period | Patients seen per clinic |
| Prince George | July 2005 - Dec 2005 | 14 | 69 | 57 | 126 | 14.0 | 9.0 |
| Kamloops | May 2000 - Dec 2005 | 41 | 182 | 282 | 464 | 13.6 | 11.3 |
| Cranbrook | Dec 2003 - Dec 2005 | 25 | 47 | 61 | 108 | 6.0 | 4.3 |
| Trail/Nelson | Dec 2003 - Dec 2005 | 31 | 79 | 83 | 162 | 7.7 | 5.2 |
| Williams Lake | Oct 2005 - Dec 2005 | 4 | 9 | 3 | 12 | n/a | 3.0 |
| All Sites | -- | 115 | 386 | 486 | 872 | n/a | 7.6 |
References
1. Grzybowski SC, Cadesky AS, Hogg WE. Rural obstetrics: A 5-year prospective study of the outcomes of all pregnancies in a remote northern community. CMAJ 1991;144:987-994. PubMed Abstract Full Text
2. Miles JE. A psychiatric outreach project to a rural community. Hosp Community Psychiatry 1980;31:822-825. PubMed Abstract
3. Darling GE, Maziak DE, Clifton JC, et al.; Canadian Association of Thoracic Surgery. The practice of thoracic surgery in Canada. Can J Surg 2004;47:438-445. PubMed Abstract Full Text
4. BC Ministry of Health. Physician compensation. www.healthservices.gov.bc.ca/pcb/forms.html (accessed 25 March 2006).
5. British Columbia Thoracic Surgery Program web site. www.thoracicsurgery.bc.ca (accessed 25 March 2006).
6. BC Provincial Health Services Authority web site. www.phsa.ca/AgenciesServices/Services/thoracic.htm (accessed 25 March 2006).
7. Bernstein M. Surgical outreach clinics in Canada: One neurosurgeon’s experience. Can J Surg 2004;47:25-28. PubMed Abstract Full Text
8. BC Ministry of Health Services. healthnetBC. http://healthnet.hnet.bc.ca (accessed 25 March 2006).
9. Aldrich JE, Rutledge JD. Assessment of PACS display systems. J Digit Imaging 2005;18:287-295. PubMed Abstract Full Text
10. Meditech Information Technology Inc. web site. www.meditech.com (accessed 25 March 2006).
11. Optimed Software Corporation web site. www.optimedsoftware.com (accessed 25 March 2006).
12. Bombin M, Harris L, Chi F, et al. Use of the emergency room in Elliot Lake, a rural community of Northern Ontario, Canada. Rural Remote Health 2004;4:240. PubMed Abstract Full Text
13. Gruen RL, Weeramanthri TS, Knight SE, et al. Specialist outreach clinics in primary care and rural hospital settings. Cochrane Database Syst Rev 2004;(1):CD003798. PubMed Abstract Full Text
14. Battye KM, McTaggart K. Development of a model for sustainable delivery of outreach allied health services to remote north-west Queensland, Australia. Rural Remote Health 2003;3:194. PubMed Abstract Full Text
15. Jong M, Kraishi M. A comparative study on the utility of telehealth in the provision of rheumatology services to rural and northern communities. Int J Circumpolar Health 2004;63:415-421. PubMed Abstract
16. Smith AC, Youngberry K, Mill J, et al. A review of three years experience using email and videoconferencing for the delivery of post-acute burns care to children in Queensland. Burns 2004;30:248-252. PubMed Abstract Full Text
17. Belmont JM, Mattioli LF. Accuracy of analog telephonic stethoscopy for pediatric telecardiology. Pediatrics 2003;112:780-786. PubMed Abstract Full Text
18. Tauber AI. Medicine, public health, and the ethics of rationing. Perspect Biol Med 2002;45:16-30. PubMed Abstract Full Text
19. Grunberg F, Williams JR. Ethical responsibilities of physicians in the allocation of health care resources. Ann R Coll Physicians Surg Can 1988;21:311-315. PubMed Citation
Michael Humer, MD, FRCSC, Andrew Luoma, MD, FRCSC, Bill Nelems, MD, FRCSC
Drs Humer, Luoma, and Nelems are members of the British Columbia Thoracic Surgery Program, located at the Interior Health Authority site in Kelowna.