Diagnosis and management of urinary incontinence in residential care
Issue: BCMJ,
vol. 55 , No. 2 , March 2013 ,
Pages 96-100 Clinical Articles
ABSTRACT: Urinary incontinence is a burdensome chronic condition afflicting a large number of elderly residents in long-term care facilities. Reversible causes commonly contribute to transient incontinence for many residents. These causes include poor fluid intake, stool impaction, depression, and the use of certain pharmaceuticals. Assessment and management in these cases can improve symptoms. Most cases of persistent incontinence have structural causes. These include impairments that lead to urge, flow, stress, and functional incontinence. As with transient incontinence, assessment and management of persistent incontinence can improve symptoms. Many other chronic conditions, such as Parkinson disease and constipation, can also contribute to loss of bladder control. Effective strategies for managing all forms of incontinence can be supported by facility policy and culture, and by staff education. Such strategies benefit elderly residents by reducing the morbidities and indignities of incontinence.
Addressing both reversible and structural causes of bladder control problems can improve the quality of life for long-term care residents.
Urinary incontinence (UI) is the involuntary loss of urine. In residential care it is extremely prevalent, affecting over half of all residents.[1] Costs associated with UI have been estimated at $5 billion per year.[2] Incontinence contributes to skin diseases, infections, and injurious falls. It also increases social isolation and profoundly affects the quality of life for both residents and caregivers alike.
Transient UI
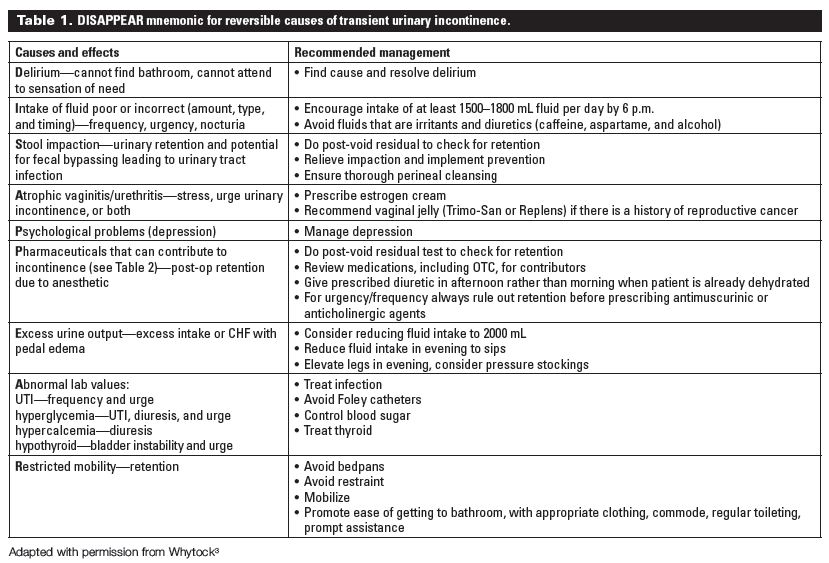
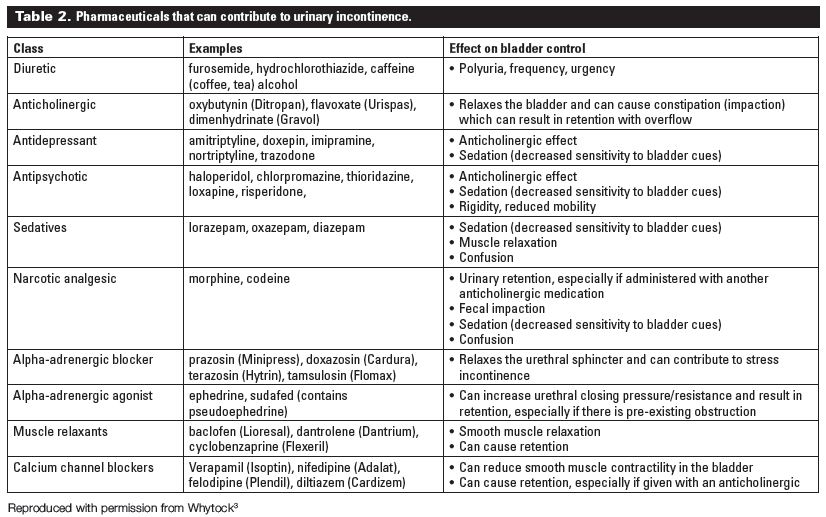
A number of UI causes do not involve a primary problem with the genitourinary system and are thus reversible. The mnemonic DISAPPEAR[3] is a helpful way to remember the causes of transient UI that are most easily remedied. These causes and management recommendations are provided in Table 1. A list of pharmaceuticals that contribute to incontinence—the second P in DISAPPEAR—is provided in Table 2.
{kind=link}
{kind=link}
When assessing a residential care patient for transient UI, a history of fluid intake should be done since some residents take in large amounts of caffeinated or diet beverages, and both caffeine and aspartame are bladder irritants. Concentrated urine from not drinking enough noncaffeinated or noncarbonated beverages can also irritate the bladder.
Evaluation for fluid shifts, such as pedal edema, should also be considered. Depression, delirium, and constipation are other conditions that can contribute to incontinence. Stool impaction in particular can cause anatomic changes that contribute to overactive bladder, urine retention, or loss of sphincter control.
Urinary and fecal incontinence are comorbid conditions that affect over 50% of elderly patients in residential care.[4] Constipation and other causes common to both types of incontinence can overlap and predispose a resident to develop dual incontinence. Fecal incontinence can also increase the risk of a symptomatic urinary tract infection, especially for female residents, due to atrophic changes and incorrect perineal cleansing. Often establishing an effective bowel protocol, including regular toileting for bowel movements, can help with this problem.
A review of symptoms and quick external observation for atrophic changes in the perineum are key to diagnosing vaginitis or urethritis, conditions common in frail postmenopausal women. Low-dose topical estrogen can often make an impact on symptoms. A quick mobility evaluation such as a timed Get Up and Go test will assess the resident’s functional ability to get to the bathroom.
Inquiring about resident ability to remove clothing in time for toilet use should be asked. Screening tests, including those measuring glucose, calcium, TSH, and renal function, and a urinalysis and culture should be done, especially in the face of recent onset or worsening incontinence. A post-void residual test to rule out retention of urine should be included in the workup.
Persistent UI
If urinary incontinence persists after assessment and management of reversible causes, the next step is to investigate and address structural causes. Table 3 describes causes of four types of persistent urinary incontinence: urge, stress, overflow, and functional incontinence.[5]
{kind=link}
Urge incontinence
Urge incontinence results from overactive bladder (OAB), a disorder characterized by symptoms of nocturia, frequency, and urgency (the immediate and urgent need to void accompanied by fear of leakage or pain). The cause of OAB is poorly understood but it is very common in the elderly and is the most common bladder abnormality in residential care.
Oxybutynin, tolterodine, darifenacin, and solifenacin are members of the antimuscarinic group of medications used to treat OAB. Oxybutynin, which is the most commonly used agent, is also the most likely to cross the blood-brain barrier and have CNS side effects. However, all antimuscarinics have the potential to cause CNS side effects in the elderly because of increased blood-brain barrier permeability, and all antimuscarinics cause other anticholinergic side effects to varying degrees. The maxim “Start low and go slow” is particularly important for these agents.
Anticholinergic side effects are very problematic in the frail elderly, causing varying degrees of dry mouth and eyes, constipation, delirium, urinary retention, dizziness, and orthostatic hypotension, which can predispose to falls.
Long-acting formulations seem more effective and better tolerated than other formulations. Many patients will experience significant side effects that may outweigh the minimal benefit derived. The choice of medication will depend on the resident’s overall goals, frailty, comorbidities, and use of other medications, especially those affecting anticholinergic load. The risk-benefit ratio for the individual must be considered.
Other important nursing interventions that should be implemented by the interdisciplinary care team in the residential care setting include timed voiding (e.g., every 3 hours) and prompted voiding (encouraging the resident regularly to try to void).
Stress incontinence
Stress incontinence occurs with any effort or exertion that increases intra-abdominal pressure, such as exercise, coughing, laughing, or lifting. This type of incontinence is very common in seniors, particularly women with poor pelvic muscle strength and tone. Kegel exercises can strengthen pelvic floor muscles. Unfortunately, Kegel exercises are difficult to teach frail seniors with any cognitive impairment. Kegel exercises also require self-motivation to be effective and must be part of a lifelong exercise program. Timed and prompted voiding are thus more practical recommendations for stress incontinence.
Overflow incontinence
Overflow incontinence results from incomplete bladder emptying due to urethral blockage, lack of bladder tone, or neurological pathway damage. Diagnosis can be made with a post-void residual urine test, either by in-and-out catheterization or, preferably, by portable ultrasound bladder scanner.
When incomplete emptying is caused by vaginal or bladder prolapse, pessary insertion can be quite effective and should be considered. Urological interventions can be attempted if retention is due to prostatic hypertrophy or urethral stricture. Surgical intervention may not eliminate incontinence in many elderly patients, but is indicated in those who are experiencing pain, discomfort, delirium, or recurrent infections.
Because urinary retention can contribute to agitation and aggression, delirium, recurrent urinary tract infections, and kidney damage, not to mention personal discomfort, overflow incontinence should be identified and managed. A urology consult should be considered if a reversible cause cannot be found. Insertion of an indwelling catheter is sometimes a necessary last resort.
Functional incontinence
Mobility and other factors that affect ease of voiding can worsen incontinence. A facility should consider basic modifications to the environment to aid continence of residents, such as appropriate placement and access to toilets and commodes. Large, colorful pictures or cartoons of a toilet at eye level rather than symbols or words are recommended, as they are more easily identified by residents with severe dementia.
Dementia and UI
Urinary incontinence is particularly common in persons with moderate to severe dementia, and is a marker of worsening disease. Indeed, UI is a significant risk factor for admission to residential care because of increased care needs.[6] There is no clear neurological cause for UI developing in individuals with dementia; rather, incontinence is likely the result of one or more sequelae of dementia.
Decreased executive function may result in poor problem-solving and planning to access the toilet. Difficulty identifying the urge to void may result in not attempting to use the toilet at all or not until it is too late. Patients with dementia become increasingly disoriented to place and time, and will sometimes forget where the bathroom is or not recognize what it is for. Consequently, this can result in voiding in inappropriate places. For example, the patient may recall voiding outdoors and see a potted plant as an appropriate place to void.
Multiple morbidities that affect mobility and function also predispose persons with dementia to incontinence. As mobility decreases with advancing dementia, the resident will increasingly find it difficult to get to the bathroom or ring for help in time. Medications that have anticholinergic effects can contribute to urinary retention and cause overflow urinary incontinence. Psychotropic drugs prescribed to manage behaviors can also increase Parkinsonian symptoms, which in turn can affect detrusor instability as well as impairing mobility and function.
Indwelling catheters and UI
Indwelling catheters are used almost exclusively for chronic urinary retention not amenable to surgical treatment or for keeping urine away from healing wounds (e.g., decubitus ulcer) on a short-term basis. Symptomatic retention (infections, pain, delirium) would be a stronger indication for catheter use than asymptomatic retention, which occasionally can be managed by accepting a higher than normal post-void residual volume.
Before considering a long-term catheter, ensure that any reversible causes are addressed, especially medications, constipation, impaction, prolapse, and irregular toileting. While an indwelling catheter can be used when skin breakdown is an issue, once any ulcers or rashes are healed, the goal should be excellent skin care that eliminates the need to use a catheter.
The benefit of close, urinary monitoring or 24-hour testing needs to be weighed against the multiple risks of catheterization. Furthermore, the risk-benefit ratio for an indwelling catheter should be evaluated in relation to urinary tract infections and repeated antimicrobial treatment. Finally, catheters are rarely necessary for end-of-life care if appropriate pain control and nursing are provided.
Conclusions
Transient and structural urinary incontinence can be effectively managed even in frail residents. Behavioral management, including effective interprofessional evaluation of incontinence, timed and prompted voiding, and addressing functional issues, can significantly improve symptoms. Moreover, better UI management requires facility-level strategies such as those outlined by Palmer,[7] including staff education and a focus on resident comfort and dignity.
Despite the prevailing attitude that incontinence is an inevitable consequence of institutionalization and aging, the senior in residential care can have a number of reversible conditions that contribute to or worsen UI. Even for those residents with persistent incontinence, facility practices can reduce the morbidities and indignities accompanying loss of bladder control and improve resident quality of life.
Competing interests
None declared.
References
1. Narayanan S, Cerulli A, Kahler KH, et al. Is drug therapy for urinary incontinence used optimally in long-term care facilities? J Am Med Dir Assoc 2007;8:98-104.
2. The Canadian Continence Foundation. Impacts of incontinence in Canada: A briefing document. May 2009. Accessed 31 March 2011. www.canadiancontinence.ca/pdf/impacts-of-incontinence.pdf.
3. Whytock S. Transient causes of urinary incontinence. In: Eyles P (ed). Promoting continence care [courseware]. Hamilton, ON: McMaster University Press; 2006: p. 23-34.
4. Leung FW, Schnelle JF. Urinary and fecal incontinence in nursing home residents. Gastroenterol Clin N Am 2008;37:697-707.
5. Miller DR. Urinary incontinence in the elderly: A clinical approach. BCMJ 1998;40:456-458.
6. Andel R, Hyer K, Slack A. Risk factors for nursing home placement in older adults with and without dementia. J Aging Health 2007;19:213-228.
7. Palmer MH. Urinary incontinence quality improvement in nursing homes: Where have we been? Where are we going? Urol Nurs 2008;28:439-444.
Dr Kow is associate head of medicine at Mount Saint Joseph Hospital, Providence Health Care. She is also residency program director in the Division of Geriatric Medicine at the University of British Columbia. Ms Carr is a clinical nurse specialist and nurse continence advisor for the Fraser Health Authority. Ms Whytock is a nurse continence advisor for the Vancouver Island Health Authority.