Building culturally safe care through connection and community
Issue: BCMJ,
vol. 68, No. 5, June 2026,
Pages 178-179 Joint Collaborative Committees
On any given day in British Columbia, a physician may travel for hours by road, air, or water to provide care in an Indigenous community. This work is deeply relational; it is shaped by trust, continuity, and cultural understanding, and it often extends beyond traditional clinical settings. While meaningful, it is also complex and can be isolating, especially when carried out in health care systems that are still evolving to support culturally safe care.
National Indigenous Peoples Day, observed in Canada annually on 21 June, offers an opportunity to reflect on these realities and the ongoing efforts to strengthen health care and address Indigenous-specific racism. The Indigenous Clinical Care Circle (ICCC) is one example demonstrating how connection, shared learning, and reflection can support physicians working in these unique contexts.
A relational network
Launched in October 2024, the ICCC is a physician-led network that brings together clinicians from across BC who provide health care to Indigenous patients, many in rural, remote, and northern communities. Rather than a formal program, the ICCC is a relational space grounded in peer support and practical learning.
The ICCC meets regularly throughout the year, with gatherings intentionally structured to reflect Indigenous cultural values. Sessions typically begin with Elder participation, territory acknowledgments, and greetings and gratitude. These elements reinforce the importance of both relationship building in clinical care and professional connection.
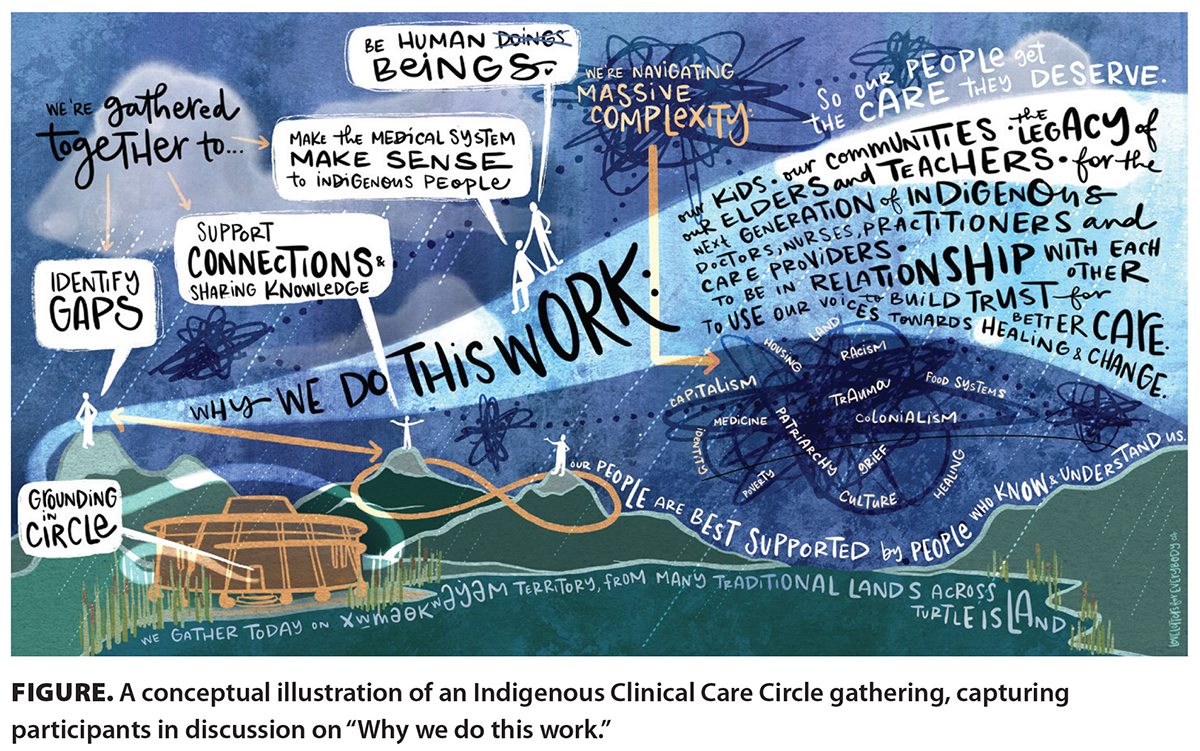
Through peer-led discussions, including “day in the life” presentations, participants share how health care is delivered across diverse community contexts. These exchanges bring to the surface practical approaches to integrating Elders, Knowledge Keepers, and traditional medicines into care. By sharing these approaches, physicians learn to create more welcoming environments for patients and their families and adapt standard care models to reflect the local, lived realities of the communities they serve [Figure].
Today, the ICCC includes approximately 35 clinicians, forming a provincial network that reduces professional isolation and strengthens culturally informed practice.
Aligning with system-wide change
The ICCC is supported through the Joint Collaborative Committees (JCCs), a partnership between Doctors of BC and the Ministry of Health. As part of a broader Indigenous-Specific Anti-Racism (ISAR) initiative, the ICCC contributes to the JCCs’ mandate to proactively dismantle racism in service delivery and improve the health care experience for Indigenous Peoples.
Insights from the ICCC highlight key areas for ongoing consideration. These include addressing travel-related barriers in remote First Nations communities, strengthening leadership and training opportunities for Indigenous physicians and trainees, and exploring compensation and funding approaches that reflect the costs of providing care in these contexts. Additional areas include supporting the integration of traditional wellness practices into clinical care; enhancing practice supports for Indigenous physicians; and enabling participation in learning, leadership, and peer-networking opportunities.
Created and guided by the JCC ISAR and Cultural Safety Steering Committee, the ICCC ensures these priorities are embedded into health care system planning. By creating a vital feedback loop, the ICCC brings forward frontline clinical experiences that can inform policy and structural change.
Understanding the realities of care
Findings from a 2025 ICCC survey of current participants further underscore these dynamics. More than 80% of respondents reported traveling long distances, often more than 4 hours, to deliver care. Many serve predominantly Indigenous patient populations within team-based models of care.
The survey also reflects a strong commitment to culturally informed care. More than half of the respondents reported incorporating Elders, Knowledge Keepers, or traditional wellness providers into their practice. Many also integrated traditional approaches alongside Western medicine, reflecting principles such as Two-Eyed Seeing.
At the same time, physicians identified ongoing challenges, including professional isolation, emotional strain, and systemic barriers. These insights reaffirm the importance of connection and support for those working in complex and underserved settings.
Advancing practice through connection
Within this context, the ICCC provides a trusted space for open dialogue, mentorship, and mutual support among physicians navigating similar complexities. Physicians describe their work as both a privilege and a responsibility, supporting communities that have experienced significant harm within colonial systems while working to improve care experiences within.
At its core, the ICCC is rooted in relationships between clinicians, with communities, and across the health care system. It reflects a simple but critical understanding: supporting those who provide care is essential to advancing culturally safe and antiracist health care systems.
To learn more about the ICCC, email isar.edi@doctorsofbc.ca.
—Terri Aldred, MD, CCFP
Family Physician, Co-Lead, Indigenous Clinical Care Circle
—Lester Todd Alec, MD, CCFP
Family Physician, Co-Lead, Indigenous Clinical Care Circle
hidden
This article is the opinion of the Joint Collaborative Committees (JCCs) and has not been peer reviewed by the BCMJ Editorial Board.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
