By: Fawziah Marra, PharmD David M. Patrick, MD, FRCPC, MHSc Mei Chong, MSc William R. Bowie, MD, FRCPC
Antibiotic use among children in British Columbia
Issue: BCMJ,
vol. 48, No. 8, October 2006,
Pages 408-409 BC Centre for Disease Control
Despite the decreasing use of antibiotics within Canada, the prevalence of antimicrobial-resistant organisms, particularly Streptococcus pneumoniae, is increasing and has become a significant threat to public health. Current evidence suggests that the use of antibiotics such as extended-spectrum penicillins, cephalosporins, and macrolides has contributed to the increasing development of resistant pneumococci. Although the data show a decline in overall prescribing of antibiotics within Canada, there are limited data on antibiotic prescribing in children within primary care. We conducted a study to characterize overall antibiotic use among children in British Columbia using population-based data.
How much antibiotic are we using?
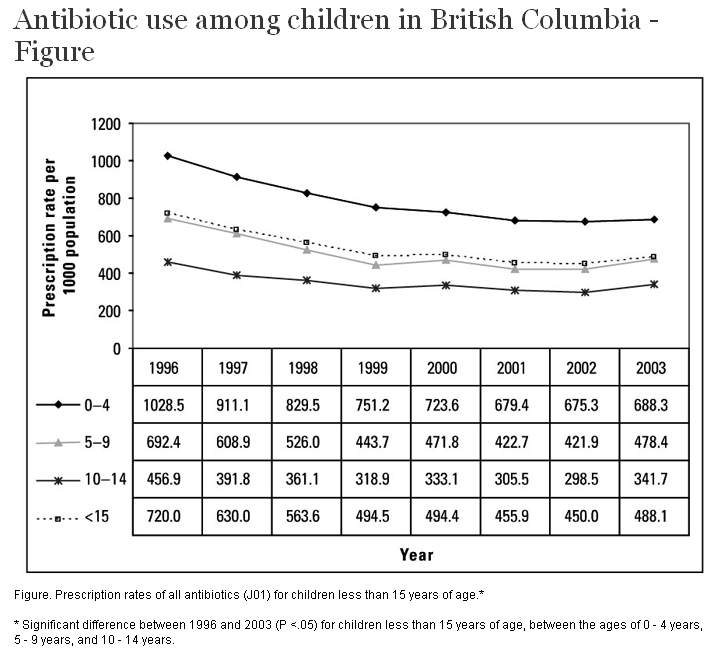
Our study showed that from 1996 to 2003, the overall BC prescription rate in children less than 15 years old decreased by one-third from 720 to 488 per 1000 children. The decrease in the rate of antibiotic consumption over time was seen across all age strata; however, the largest decrease (33%) was seen in children between 0 and 4 years old (Figure).
{kind=link}
What types of antibiotic are we using?
For all children less than 15 years of age, the largest decrease in consumption rate (63%) was seen with trimethoprim/sulfamethoxazole (Table). The consumption rate of beta-lactams (i.e., penicillins and cephalosporins) also decreased significantly over time. In 1996, the rate of penicillin use was 414 prescriptions per 1000 children, but fell by 40% to 249 prescriptions per 1000 children in 2003. Similarly for the cephalosporins, the rate decreased by 30% from 106 per 1000 children in 1996 to 74 per 1000 children in 2003. This trend of decreasing antibiotic use was seen in all age groups but the greatest decline was in the age category of 0 to 4 years. Consumption rate of tetracyclines has remained relatively stable over the 7-year study period (3.6 per 1000 children in 1996 to 3.7 per 1000 children in 2003) and 99% of tetracycline use was contributed by the 10- to 14-year-old children.
{kind=link}
The rate of antibiotic consumption increased for both the macrolide and quinolone antibiotic classes. From 1996 to 2003, macrolide consumption increased by 24% (102 to 126 prescriptions per 1000 children) and this was reflected in all three age stratifications, with the greatest increase seen in the 0- to 4-year-olds (44% increase for 0- to 4-year-olds; 19% increase in the 5- to 9-year-olds; and 12% increase in the 10- to 14-year-olds). Quinolone consumption also increased over the 7-year study period from 0.59 to 0.84 prescriptions per 1000 children (i.e., 42%), however the increasing trend for quinolones was only significant for age groups 5 to 9 (15%) and 10 to 14 (36%).
In BC, extended spectrum penicillins account for the majority of antibiotic use within the class of penicillins (Table). In 2003, extended spectrum penicillins (e.g., amoxicillin and ampicillin) accounted for 85% of penicillin prescriptions, while the beta-lactamase sensitive penicillins (e.g., penicillin V) were used 6% of the time and combinations of penicillins (e.g., amoxicillin/clavulanate) account for 5% of all penicillin prescriptions. 1n 1996, erythromycin use accounted for 83 prescriptions per 1000 children. But this has declined significantly and in 2003, the erythromycin prescription rate was 23 per 1000 children (-72%). In contrast, use of clarithromycin increased by 269% from 18.2 (1996) to 67.0 (2003) prescriptions per 1000 children (P <.001). Use of azithromycin has also increased from 0.4 prescriptions per 1000 children to 34.9 prescriptions per 1000 children (an increase of 8056%).
What indications are we using antibiotics for?
The Table shows the change in population-based rates of antibiotic prescribing for each condition over the 7-year study period. From 1996 to 2003, antibiotic prescribing rates decreased significantly for all indications except treatment of pneumonia, which saw an increase in prescribing rates. The largest decrease was seen in the use of antibiotics for the treatment of acute otitis media (decreased by one-half by 2003). In 1996, use of antibiotics for upper respiratory tract infection (URTI) was the second most common indication, but by 2003 it was the most common reason for antibiotic prescriptions in children less than 15 years of age, particularly for acute pharyngitis (41 prescriptions per 1000 children), and tonsillitis (24 prescriptions per 1000 children). Antibiotic prescriptions for treatment of bronchitis also declined by approximately one-third in the 7-year time frame; the majority of this was accounted for by a decrease in prescriptions for acute bronchitis and bronchiolitis (-36%). All three cohorts of children had a substantial drop in the rate of antibiotic prescribing for acute otitis media, bronchitis, and URTI. The decrease in antibiotic prescribing rates was similar across the three age groups, ranging from 25% to 48%. In contrast, antibiotic prescribing increased in all three age groups for the treatment of pneumonia, with the largest increase seen in the 0- to 4-year-olds (39%).
Conclusions
Although overall antibiotic use has declined in children, there is increased use of macrolides, particularly clarithromycin and azithromycin, which may have ramifications on macrolide-resistant streptococci, including Streptococcus pneumoniae and group A streptococci. In addition, a large proportion of antibiotic use in children is for URTI and bronchitis; indications where there is a high likelihood that the cause is viral rather than bacterial.
—Fawziah Marra, PharmD, FCSHP
—David M. Patrick, MD, MHSc, FRCPC
—Mei Chong, MSc
—William R. Bowie, MD, FRCPC
BC Centre for Disease Control