Preoperative rectal cancer imaging
Issue: BCMJ,
vol. 45 , No. 6 , July August 2003 ,
Pages 259-261 Clinical Articles
Preoperative imaging studies are necessary for recommending preoperative adjuvant therapy and surgical approach when treating rectal cancer. We discuss the utility of endorectal ultrasound, magnetic resonance imaging, and CT imaging for the assessment of rectal cancer. All patients should have CT for metastatic staging. The majority of patients should have magnetic resonance imaging to assess pelvic staging of tumor invasion, lymph nodes, and relationship of the tumor to adjacent pelvic structures. Endorectal ultrasound is useful to assess whether superficial cancers in the distal rectum should be locally excised.
Preoperative imaging is mandatory to assess cancer staging with respect to recommendation of type of surgical procedure and neo-adjuvant therapy. In this paper, we discuss the accuracy of endorectal ultrasound, magnetic resonance imaging (MR), and computed tomography (CT) for staging rectal cancer and make recommendations for preoperative imaging studies.
Endorectal ultrasound, magnetic resonance imaging, and CT imaging all have useful roles to play when assessing rectal cancer.
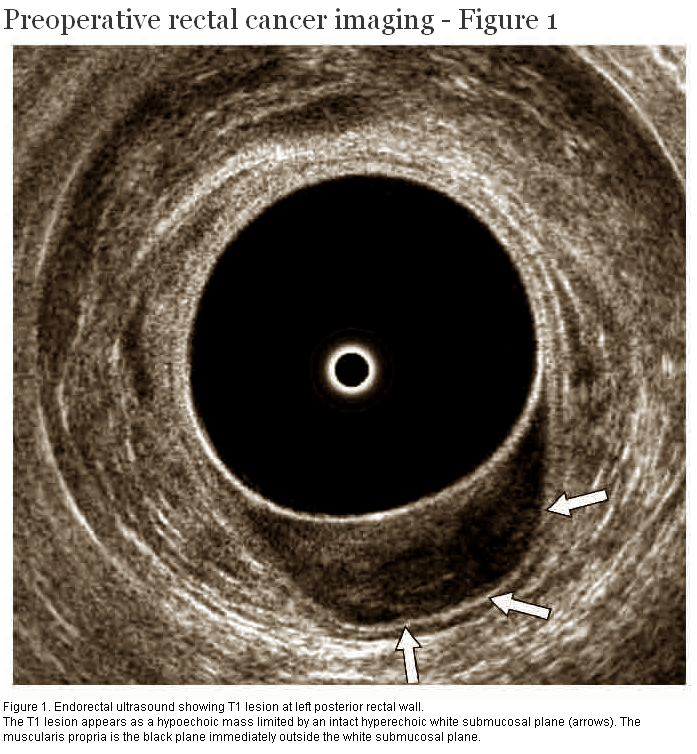
Endorectal ultrasound is valuable for local staging because it provides excellent anatomical definition of bowel wall layers. Carcinoma appears hypoechoic with variable through transmission on ultrasonography. A T1 tumor is diagnosed when muscularis mucosa is hypoechoic but echogenic submucosa separates the lesion from muscularis propria (Figure 1). Hypoechoic thickening of muscularis propria indicates T2 extension. T3 extension is indicated by hypoechoic tumor extension into perirectal fat. Endorectal ultrasound can identify preservation of the fat plane between an anterior rectal cancer and prostate, seminal vesicles, or vagina. Endorectal ultrasound can also identify invasion of levators and anal sphincter.
{kind=link}
Accuracy of endorectal ultrasound for determining local extent of rectal carcinoma is 80% to 90%.[1] Strengths of this type of imaging include high spatial resolution and good differentiation between layers of the bowel wall. The major pitfall of endorectal ultrasound is overstaging of T2 tumors as T3 lesions due to inflammation, fibrosis, radiation, and postbiopsy hematoma. However, there are subtle sonographic characteristics that aid in the distinction of the tumor from these entities. For example, fibrotic change is more likely to have a strand-like appearance, and exhibit less through transmission than carcinoma. Understaging may also occur at any stage secondary to microscopic nests of neoplastic cells beyond the main tumor margin. Technical difficulties—including stricturing and upper location of rectal tumors—can prevent accurate staging.
Overall accuracy of endorectal ultrasound for assessing malignant lymph nodes is 75% to 85%.[2] Malignant perirectal nodes are well-defined, round, and hypoechoic. Benign nodes are typically oval and small (size less than 4 mm).
Magnetic resonance imaging
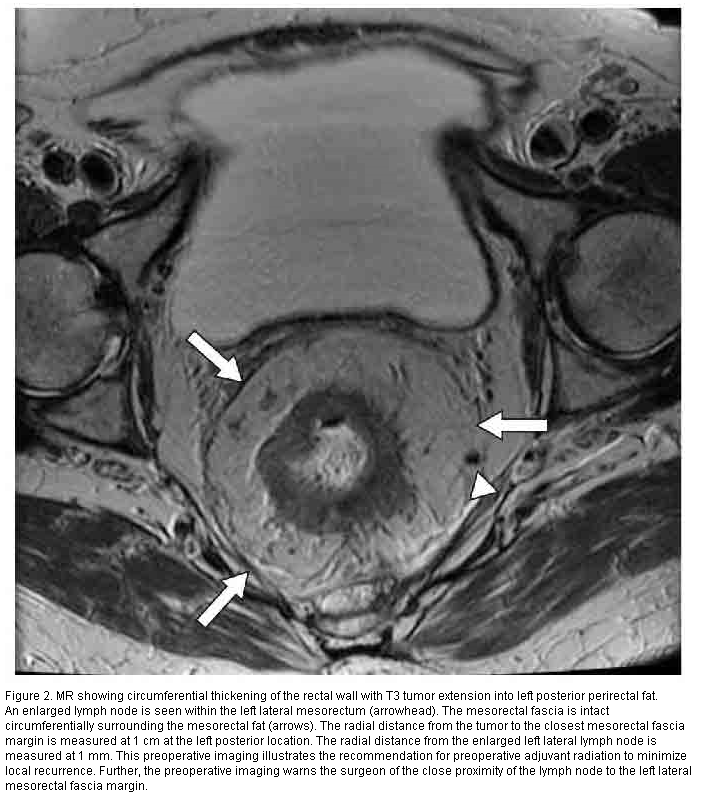
Magnetic resonance is valuable for local staging because it provides multiplanar imaging, visualization of the rectal wall layers, and tumoral enhancement. Rectal cancer has a low signal on T1-weighted images and enhances strongly with administration of gadolinium, an MR contrast agent. T1 stage is diagnosed in the presence of thickening of the muscularis mucosa with preservation of submucosal plane. T2 stage is diagnosed when thickening of the low-signal muscularis propria is visualized (Figure 2). T3 staging is diagnosed when the tumor penetrates the entire thickness of the bowel wall and invades the perirectal fat. T4 stage is diagnosed when the enhancing tumor invades adjacent muscles and organs.
{kind=link}
MR accuracy of T-staging is 80%. Accuracy is improved to 90% using gadolinium and dynamic sequences. Peritumoral inflammatory change and fibrotic change can be differentiated from true T3 stage because of a lack of enhancement, but this distinction remains difficult. Accuracy of T4 invasion of adjacent muscles and organs is 80%, a particular strength of MR compared to CT and ultrasound. Coronal imaging is particularly valuable in characterizing pelvic floor invasion for assessment of sphincter preservation.
Accuracy of MR for assessing lymphadenopathy is 60% to 80%,[3] not as high as ultrasound. However, coronal MR has the advantage of being able to visualize obturator nodes.
Another advantage of MR is that it allows evaluation of mesorectal fascia that appears hypointense on T1-weighted images (Figure 2). A margin of 5 mm between the nearest tumor and the mesorectal fascia has been shown to predict clear resection margins after total mesorectal excision. Ability to predict clear resection margins affects the recommendation for either neo-adjuvant short-course preoperative radiation or long-course chemoradiation.
CT
The primary function of CT is detecting distal spread, especially to the liver and lung bases.[4] Accuracy of CT for staging the extent of local spread is limited by its inability to resolve layers of the bowel wall. However, CT is useful for visualizing the invasion of local structures. Pelvic, portal, and paraortic adenopathy can be assessed using CT. CT demonstrates excellent sensitivity for detecting macroscopic tumor deposits in the liver (Figure 3), but ultrasound may be necessary to distinguish a cancer from a simple liver cyst.
{kind=link}
Recommendations for rectal cancer staging
CT of the abdomen and pelvis is the test of choice for evaluating distal spread. It is the most sensitive modality for detecting liver metastases. In addition, it is effective in evaluating the other abdominal organs, lung bases, and lymph node chains for metastatic spread.
MR or endorectal ultrasound are excellent modalities for the staging of local disease. MR has additional benefits for staging T4 lesions, evaluating the pelvic floor, and predicting clear total mesorectal excision margins. Endorectal ultrasound is more sensitive in detecting local lymph node enlargement and in the T assessment of distally located tumors.
Therefore, a combination of CT with either MR or endorectal ultrasound for local staging is currently recommended. The relationship of radial margins of the rectal cancer to the mesorectal fascia increases the importance of MR in assessing local staging.
Competing interests
None declared.
References
1. Kim NK, Kim MJ, Yun SH, et al. Comparative study of transrectal ultrasonography, pelvic computerized tomography, and magnetic resonance imaging in preoperative staging of rectal cancer. Dis Colon Rectum 1999;42:770-775. PubMed Abstract
2. Sunouchi K, Sakaguchi M, Higuschi Y, et al. Limitations of endorectal ultrasonography: What does a low lesion more than 5 mm in size correspond to histologically? Dis Colon Rectum 1998;41:761-764. PubMed Abstract
3. Kwok H, Bissett IP, Hill GL. Preoperative staging of rectal cancer. Int J Colorectal Dis 2000;15:9-20. PubMed Abstract Full Text
4. Heriot AG, Grundy A, Kumar D. Preoperative staging of rectal carcinoma. Br J Surg 1999;86:17-28. PubMed Abstract Full Text
David Malfair, MD, Jacqueline A. Brown, MD, and P. Terry Phang, MD
Dr Malfair is a resident in the Department of Radiology at the University of British Columbia. Dr Brown is a radiologist at St. Paul’s Hospital in Vancouver and an assistant professor in the Department of Radiology at the University of British Columbia. Dr Phang is a colorectal surgeon at St. Paul’s Hospital and an associate professor in the Department of Surgery at UBC.