Practice patterns and appropriateness of rectal cancer management in British Columbia
Issue: BCMJ,
vol. 45 , No. 7 , September 2003 ,
Pages 324-329 Clinical Articles
Survival and recurrence rates for all rectal cancers in BC in 1996 were suboptimal relative to reports from other centres. From chart reviews, questionnaire mail-outs, and telephone calls, we now report possible factors which could result in suboptimal outcomes, including suboptimal staging investigations, surgical procedures, and adjuvant radiation and chemotherapy.
Staging investigations performed within 3 months of diagnosis were as follows: chest X-ray in 65% of patients, barium enema or colonoscopy in 74% of patients, CT scan in 21% of patients, ultrasound in 42% of patients, and endorectal ultrasound in 3% of patients.
Adequacy of resection was judged by use of total mesorectal excision as the preferred surgical resection technique and by pathologic assessment of the radial resection margin. Whether total mesorectal excision was performed could not be reliably determined from operative reports. Radial resection margins were assessed in only 48% of pathology reports.
Adjuvant radiation was given in 60% and adjuvant chemotherapy in 60% of stage 2 and stage 3 tumors.
These data show that in BC there is suboptimal cancer staging by use of staging investigations and pathology reporting. Surgical techniques and use of adjuvant therapy are also suboptimal. As such, we have identified potential opportunities for improving outcome including improved use of staging investigations preoperatively, improved use of preoperative adjuvant radiation, postoperative adjuvant chemotherapy, and improved surgical techniques and pathology reporting.
Our local recurrence rates for rectal cancer are higher than recent reports from centres that use preoperative adjuvant radiation and mesorectal excision. As much as possible, we need to prevent pelvic recurrence, which can result in a slow and painful death.
Rectal cancer outcomes are dependent on stage of cancer and appropriate management. The most important management that determines outcome is adequacy of surgical resection. Adjuvant radiation and chemotherapy also have an influence on the outcome. We have previously reported 1996 rectal cancer outcomes in BC.[1] We found that survival and recurrence rates were suboptimal relative to more recent reports from other centres.[2-4]
The British Columbia Cancer Agency (BCCA) provided guidelines for the management of rectal cancer based on the consensus guidelines published by the National Institutes of Health.[5] Adjuvant postoperative radiation and chemotherapy were recommended to decrease local recurrence rates for stage 2 and stage 3 rectal cancers (Table 1). Preoperative chemoradiation was recommended for fixed tumors of borderline resectability followed by postoperative chemotherapy.
In this study we report the outcomes of survival and local recurrence in relation to use of staging investigations, adequacy of surgical procedure to resect the cancer, and use of adjuvant radiation and chemotherapy. Finally, we comment on our outcomes relative to other centres and to assess whether we were appropriately investigating and managing rectal cancer according to the guidelines written by the BC Cancer Agency.
We conducted a retrospective review of all rectal cancers in British Columbia in the calendar year of 1996. All cancers of the rectum or rectosigmoid junction were identified from the BC Cancer Registry. A total of 495 cases were identified as rectal or rectosigmoid adenocarcinoma, diagnosed in a BC resident in 1996 and treated in BC. Information was judged too incomplete for analysis in 14 cases, leaving 481 cases that could be evaluated. These 14 cases were subjects who were not referred to the BC Cancer Agency and whose responsible physicians at the time of diagnosis could not be contacted.
Clinical data were abstracted from BCCA charts for the 45% of patients who were referred to the agency for treatment or follow-up. For the 55% of patients who were not referred to the agency, data were obtained from a questionnaire sent to family doctors and surgeons identified from Cancer Registry records. Data were abstracted from the medical charts or questionnaires by investigators (PTP, JM, RHT, RC, ND, JH, GM, and BS) and checked for completeness and consistency by medical record analysts (CS and JP). Data inconsistencies were resolved by contact with treating physicians and hospitals.
TMN staging was performed using pathology, diagnostic, and operative reports. Disease-specific survival, local recurrence, and overall recurrence (local and distant) data are reported at 4 years.
Data are recorded as mean and range. Statistics were performed using SPSS software (version 9.0, Chicago, IL). Methods of comparison included the Pearson chi-square test for categorical data comparisons and the log-rank test for comparisons involving time-to-event data (e.g., survival, recurrence). Survival and time-to-recurrence curves were plotted using the Kaplan-Meier method (product-limit method).
Of 481 cases that we could evaluate, median age was 70; 42.7% were female and 57.3% were male.
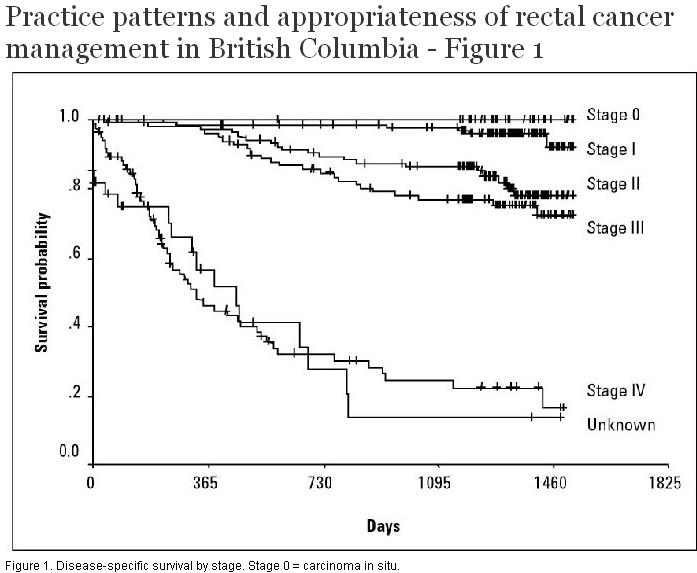
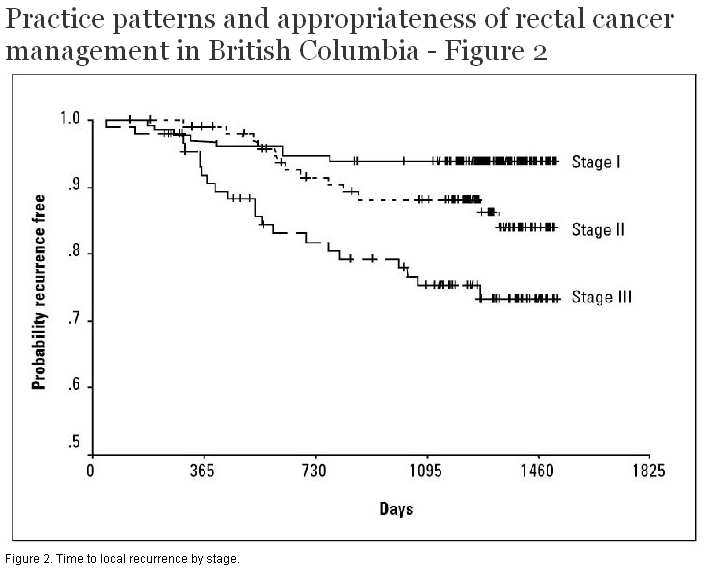
Four-year disease-specific survival was dependent on stage (Figure 1). Stage 1 cancer had a 91% survival (n = 134) and in situ cancer had a 100% survival (n = 29). In contrast, stage 4 cancer had a 17% survival rate (n = 83). Stage 2 and stage 3 cancers had survival rates of 78% and 72%, respectively (n = 107, 100). There were 28 cancers for which staging information was unknown. This group with unknown stage had a 15% survival rate. At 4 years, local recurrence rates were 0% for in situ cancer, 7% for stage 1, 16% for stage 2, and 27% for stage 3 (Figure 2). At 4 years, overall recurrence rates (local and distant) were 9% for stage 1, 28% for stage 2, and 40% for stage 3.
{kind=link}
{kind=link}
Use of staging investigations performed within 3 months of diagnosis were as follows: chest radiographs were performed in 65% of cases, colonoscopy or barium enema in 74%, CT scans in 21%, abdominal ultrasound in 42%, and endorectal ultrasound in 3% (Table 2).
Most rectal cancers were resected; 51% by anterior resection, 33% by abdominoperineal resection, 5% by Hartmann’s procedure, and 0.6% by proctocolectomy (in association with ulcerative colitis). Local excision and polypectomy were each performed in 5% of rectal cancers. Abdominoperineal resection was performed in 29% of cancers located 5 cm to 10 cm from the anus in the midrectum.
Adequacy of resection could not reliably be judged from operative or pathology reports. Key phrasing of total mesorectal excision and wide resection margins (proximal, distal, radial) were not often used in operative reports. Twenty percent of pathology reports did not contain assessment of proximal and distal resection margins. There was no comment on radial margins in 52% of pathology reports.
Local excision was performed in 16 cancers, of which 15 were T1 and one was T2. Postoperative radiation was given in 11 patients. Two patients had local recurrence (12.5%). One patient who had local recurrence received chemoradiation followed by salvage abdominoperineal resection. That patient is alive without disease. The second patient who had local recurrence was elderly (age 84) and deemed unfit to receive radiation. He died with recurrent cancer.
Forty-two hospitals participated in rectal cancer surgery in 1996, of which 16 hospitals performed five or fewer rectal cancer operations; eight hospitals performed six to nine rectal cancer operations; 18 hospitals performed 10 or more rectal cancer operations. A total of 145 surgeons performed rectal cancer surgery, of which 121 performed five or fewer operations; 22 surgeons performed six to nine operations; two surgeons performed 10 or more operations.
Adjuvant radiation was given to 60% of patients with stage 2 and stage 3 cancers within 15 cm of the anus (Table 3). The majority (89%) received postoperative radiation while a few (11%) received preoperative radiation. Of the patients who did not receive adjuvant radiation, 16% were unfit or refused and in 24% there was no reason stated for not giving adjuvant radiation. Adjuvant chemotherapy was given to 60% of stage 2 and stage 3 cancer patients. Of the 40% of patients who were eligible for but did not receive adjuvant chemotherapy, 11% were unfit, while no reason was stated in 29%. We found that the proportions of patients who had to drive less than 2 hours (75%) or more than 2 hours (25%) to regional cancer centres were similar for the groups that received and did not receive adjuvant radiation (P < 0.4) and chemotherapy (P < 0.4).
For stage 2 and stage 3 rectal cancers, British Columbia’s disease-free survival rates are 78% and 72% respectively, and our local recurrence rates are 16% and 27%, respectively, at 4 years. As such, our survival and local recurrence rates are inferior to local recurrence rates of less than 10% from other centres.[2-4] On the strength of improved local recurrence rates using new protocols from these centres, we now recommend the use of preoperative adjuvant therapy over postoperative adjuvant therapy. From our review of practice patterns in 1996, we have identified potential opportunities for improving outcome including improved use of staging investigations, improved use of preoperative adjuvant radiation and chemotherapy, and improved surgical techniques and pathology reporting.
After making the diagnosis of rectal cancer, the next step in management should be staging investigations to guide the use of preoperative adjuvant radiation and chemotherapy and the type of surgical procedure. We found that a substantial number of patients did not receive staging investigations including chest X-ray or abdominal ultrasound, widely available tests even in smaller communities. Most patients did undergo colonoscopy or barium enema for assessment of synchronous colon lesions. Few patients were staged using CT or endorectal ultrasound.
One potential opportunity to improve outcome may be to use preoperative rather than postoperative adjuvant therapy. Postoperative adjuvant radiation and chemotherapy was advocated in the 1990 consensus statement by the National Institutes of Health.[5] That consensus statement was guided by results from the Gastrointestinal Tumor Study Group, 1986, and the North Central Cancer Treatment Group, 1991,[6,7] which showed that postoperative radiation and chemotherapy decreased local pelvic recurrence rates (24% to 11% and 25% to 14%, respectively) but did not improve survival. More recently, studies of preoperative adjuvant radiation have shown similar decrease in local recurrence and, moreover, increased survival. In one Swedish rectal cancer trial, a short course of preoperative radiation resulted in decrease in local recurrence from 27% to 12% and increased 5-year survival from 48% to 58%.[8] A recent report from the Dutch total mesorectal excision (TME) trial had local recurrence rates of 2.4% using short-course preoperative radiation.[4] Two North American studies using long-course preoperative radiation and chemotherapy have excellent 5-year outcomes, with local recurrence of 4% and 5% and survival of 85% and 93%.[2,3] Therefore, preoperative short-course radiation or long-course radiation and chemotherapy have potential for improving local recurrence and survival compared to postoperative adjuvant therapy. In consideration of these studies that indicate a possible advantage for preoperative radiation, the BC Cancer Agency has endorsed increasing the use of preoperative radiation. Recent guidelines on this subject are published on their web site (www.bccancer.bc.ca/HPI/CancerManagementGuidelines/Gastrointestinal/06.Rectum/default.htm), Table 1.
In view of these data favoring preoperative over postoperative adjuvant therapy, preoperative staging investigations are essential to guide use of preoperative adjuvant therapy. We need to alter practice patterns in our management of rectal cancer to promote the use of preoperative staging investigations and increased use of preoperative adjuvant therapy. Since preoperative short-course radiotherapy is less resource-intensive than postoperative long-course radiotherapy, increased use of preoperative short-course radiotherapy could improve access to adjuvant radiotherapy.
After cancer stage, surgical technique is likely the most important factor to affect outcome. Dr Bill Heald has promoted widespread interest in the surgical technique of mesorectal excision while Dr Phil Quirke has increased appreciation of pathologic examination of the rectal cancer specimen in relation to the mesorectal circumferential margin.[9,10] Groups in Europe and North America have published excellent results from mesorectal excision with local recurrence rates of less than 10%.[11-13] Our local recurrence rates of 16% and 27% for stage 2 and stage 3 cancers, respectively, are well above 10%. By implication relative to results reported for mesorectal excision, our surgical technique is likely not an intact mesorectal excision in many cases. However, we were unable to determine clearance of radial margins or intactness of the mesorectal fascial envelope from operative or pathology reports. Key phrases including mesorectal excision and wide resection margins (proximal, distal, radial) were lacking in most operative reports. Assessment of radial margins was not stated in 52% of pathology reports. Clearly, we need to improve operative and pathology reporting relative to mesorectal excision and resection margins. Our rate for abdominoperineal resection of 29% for midrectal cancers may be considered high by surgeons trained to perform total mesorectal excision, a technique that requires complete proctectomy and reconstruction by coloanal anastomosis. By inference from our high local recurrence rates, we need to improve our surgical technique of mesorectal excision.
Guidelines for pathology staging of surgical rectal cancer specimens recommend a minimum of 12 lymph nodes to determine that there are no regional lymph node metastases.[14,15] However, the average number of lymph nodes examined was six, and there is wide variation in the number of lymph nodes examined (range 0 to 21). Just as there is increasing acceptance of mesorectal excision as a standardized surgical technique, there also needs to be a standardized technique of examination and reporting of the surgical specimen resulting from mesorectal excision.[10,16] In addition, we wish to recommend using the R0, R1, R2 designation for residual disease absent or present microscopic or macroscopic[17] as a prognostic indicator with significance similar to cancer stage. The pathology report is key to staging, recommendation of postoperative adjuvant therapy, and potential benefit to outcome resulting from appropriate adjuvant therapy.
We need to improve our outcomes in the setting of a large geographic area, 42 participating hospitals, 137 general surgeons, and four regional cancer centres. Our group proposes an education program for surgeons and pathologists in our province. The objective is to teach and standardize the surgical technique of mesorectal excision and pathology examination of the rectal cancer specimen. In order to increase the use of preoperative adjuvant radiation, we will have to educate and improve access to preoperative staging investigations and preoperative adjuvant radiation facilities. Experience elsewhere suggests that results in rectal cancer can be improved by surgical specialization and coordinated multidisciplinary management.[2-4,9-13] As such, cooperative groups and a standardized systems approach are required to achieve the excellent results reported from other centres treating rectal cancer. Consideration should be given to restriction of rectal cancer surgery to surgeons trained for total mesorectal excision and to hospitals with sufficient volumes to support rectal cancer surgery programs.
In summary, our local recurrence rates for rectal cancer management are higher than recent reports from centres that use preoperative adjuvant radiation and mesorectal excision. As much as possible, we need to prevent pelvic recurrence, which can result in a particularly slow and painful death. Potential strategies for improving our outcomes include increased use of staging investigations and increased use of preoperative radiation and mesorectal excision.
Competing interests
None declared.
Table 1. Guidelines for adjuvant therapy for rectal cancer.
| Pre-op adjuvant therapy | Post-op adjuvant therapy | |
| 1996 | Clinically fixed tumors receive 5-week pre-op chemoradiation | Stage 2 and stage 3 cancers receive 5-week post-op radiation with 6 month chemotherapy |
| 2002 | Clinically fixed tumors receive 5-week pre-op chemoradiation Pre-op imaged mobile stage 2, and stage 3 tumors receive 1 week pre-op radiation |
Stage 3 cancers receive 6 month post-op chemotherapy |
Table 2. Use of preoperative staging investigations for rectal cancer in British Columbia, 1996.
|
Chest X-ray 65% |
Table 3. Use of adjuvant radiation and chemotherapy for rectal cancer in British Columbia, 1996.
|
|
Given | Not given – Patient unfit or refused |
Not given – Reason unknown |
| Adjuvant radiation | 60% | 16% | 24% |
| Adjuvant chemotherapy | 60% | 11% | 29% |
References
1. Phang PT, MacFarlane J, Taylor RH, et al. Effects of positive resection margin and tumor distance from anus on rectal cancer treatment outcomes. Am J Surg 2002,183:504-508. PubMed Abstract Full Text
2. Chari RS, Tyler DS, Anscher MS, et al. Preoperative radiation and chemotherapy in the treatment of adenocarcinoma of the rectum. Ann Surg 1995;221:778-787. PubMed Abstract
3. Stryker SJ, Kiel KD, Rademaker A, et al. Preoperative chemoradiation for stages II and III rectal carcinoma. Arch Surg 1996;131:514-519. PubMed Abstract
4. Kapiteijn E, Marijnen CAM, Nagtegall ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 2001;345:638-646. PubMed Abstract Full Text
5. NIH Consensus Conference: Adjuvant therapy for patients with colon and rectal cancer. JAMA 1990;264:1444-1450. PubMed Citation
6. Gastrointestinal Tumor Study Group. Prolongation of the disease-free interval in surgically treated rectal carcinoma. N Engl J Med 1985;312:1465-1472. Abstract
7. Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991;324:709-715. PubMed Abstract
8. [No authors listed.] Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med 1997;336:980-987. Erratum in: N Engl J Med 1997;336:1539. PubMed Abstract Full Text
9. Heald RJ, Moran BJ, Ryall RDH, et al. Rectal cancer, the Basingstoke experience of total mesorectal excision, 1978 - 1997. Arch Surg 1998;133:894-899. PubMed Abstract Full Text
10. Quirke P, Durdey P, Dixon MF, et al. The prediction of local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumor spread and surgical excision. Lancet 1986;2:996-999. PubMed Abstract
11. Martling AL, Holm T, Rutqvist LE, et al. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet 2000;356:93-96. PubMed Abstract Full Text
12. Merchant NB, Guillem JG, Paty PB, et al. T3N0 Rectal cancer: Results following sharp mesorectal excision and no adjuvant therapy. J Gastrointest Surg 1999;3:642-647. PubMed Abstract Full Text
13. Zaheer S, Pemberton JH, Farouk R, et al. Surgical treatment of adenocarcinoma of the rectum. Ann Surg 1998;227:800-811. PubMed Abstract Full Text
14. Goldstein NS, Sanford W, Coffey M, et al. Lymph node recovery from colorectal resection specimens removed for adenocarcinoma: Trends over time and a recommendation for a minimum number of lymph nodes to be removed. Am J Clin Pathol 1996;106:209-216. PubMed Abstract
15. American Joint Committee on Cancer. Manual for Staging of Cancer. Philadelphia, PA: JB Lippincott, 1992:75-82. www.cancerstaging.org.
16. Adam IJ, Mohamdee MO, Martin IG, et al. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet 1994;344:707-711. PubMed Abstract
17. Hermanek P, Wittekind C. The pathologist and the residual tumor, R, classification. Path Res Pract 1994;190:115-123. PubMed Abstract
P. Terry Phang, MD, John K. MacFarlane, MD, FRCSC, Robert H. Taylor, MD, FRCSC, Rona E. Cheifetz, MD, FRCSC, Noelle Davis, MD, John H. Hay, MB, Greg McGregor, MD, FRCSC, Caroline Speers, BA, Barry J. Sullivan, MD, FRCSC, Janet Pitts, BA, CHRA(C), and Andrew J. Coldman, PhD
Dr Phang is a colorectal surgeon at St. Paul’s Hospital in Vancouver and an associate professor in the Department of Surgery at the University of British Columbia (UBC). Dr MacFarlane is a professor of surgery at UBC and practises at St. Paul’s Hospital. Dr Taylor is staff general surgeon at Mount St Joseph Hospital. Dr Cheifetz is an assistant professor of surgery at UBC and practises at Vancouver Hospital and Health Sciences Centre. Dr Davis is an associate professor of surgery, UBC, and director of the BCCA Surgical Oncology Network. Dr Hay is a radiation oncologist at the BC Cancer Agency Vancouver Cancer Centre. Dr McGregor is a clinical professor of surgery at UBC and practises at Vancouver Hospital. Ms Speers is a data manager at the BCCA’s Breast Cancer Outcomes Unit. Dr Sullivan is staff general surgeon at the Kelowna General Hosptial. Ms Pitts is a data manager at the BCCA. Dr Coldman is head of Population and Preventive Oncology at the BCCA.