The patient-centred interview and international medical graduates: A preliminary view
Issue: BCMJ,
vol. 51 , No. 6 , July August 2009 ,
Pages 246-249 Clinical Articles
As medicine is both an art and a science, the clinical care of a patient depends on both scientific and personal factors. These personal factors can only be addressed in a medical interview, currently referred to as the “patient-centred approach.” Medical schools are giving increasing emphasis to the patient-centred approach, thus Canadian-trained physicians of the future will be increasingly aware of such principles. However, as Canada opens its doors more widely to international medical graduates, we must ensure that these graduates appreciate and are skillful in the patient-centred approach. We describe the experience of one international medical graduate (the primary author) in acquiring patient-centred interviewing skills, and the outcomes. We also describe the positive effect of his experience—in that colleagues in his study group also benefited from his newfound knowledge, skills, and improved attitude. Enhancing the interviewing skills of foreign-trained doctors upgrades their skills to the levels taught by Canadian medical schools, helps graduates pass requisite examinations, and improves patient care.
Many IMGs appear to lack the basic training in communication skills that Canadian medical students receive, but a focused mentorship program can produce striking results.
One has a greater sense of intellectual degradation after an interview with a doctor than from any human experience,” stated Alice James (1848–1892), sister of novelist Henry James and philosopher William James.[1] Several decades later, in 1927, Dr Francis Peabody wrote, “The treatment of a disease may be entirely impersonal; the care of a patient must be completely personal.”[2]
These sentiments highlight the importance of making the medical interview as pleasant and meaningful as possible. Medical interviewing is an art and a science; it can be taught and learned. When a patient consults a doctor, the patient and the doctor each have their own agenda, but it behooves the doctor to be sensitive to the patient’s agenda. Such an approach is called “patient-centred interviewing.”[3] In Canada, medical students are required to be familiar with the concept of patient-centred interviewing. Indeed, in examinations of medical students and residents using the objective structured clinical examination (OSCE) candidates’ communication skills are evaluated.
In British Columbia, the need for more doctors[4] means that international medical graduates (IMGs) are being afforded an opportunity to access the Canadian Resident Matching Service (CaRMS).[5] However, to do so, IMGs must also take the OSCE. IMGs appear to lack the basic training in communication skills that Canadian medical students commonly receive, and this may be one reason that IMGs do less well in objective structured clinical examinations.
My coauthor and I have direct experience of the enhancement of communication skills possible, having worked together as trainer (JB) and trainee (TK). Before coming to British Columbia, I was a practitioner in Egypt for 13 years. My training in communication skills with JB resulted in immense personal growth and professional transformation. This experience is worth considering along with data from an audit of the training experience and examination results of some other IMGs.
Transformation
I first became interested in correcting the flaws in my interview style after I failed to pass a clinical examination in 2007—the IMGBC OSCE. I needed to pass that examination to become eligible to apply for a family medicine residency in British Columbia. I had already passed the Medical Council of Canada Qualifying Exam (MCCQE) Part 1, but that examination assessed only medical knowledge and not physician-patient interaction.
I was ill-prepared for the IMGBC clinical examination and I failed. Dr Rodney Andrew, the director of the IMGBC program, told me in his feedback that I was asking too many questions too quickly, using too many leading questions, and not listening to the patient. This valuable information helped me gain insight on my weakness and spurred me on to change. I realized that I needed to enhance my interview skills in order to pass the IMGBC clinical examination and to be successful in other exams, such as MCCQE Part 2, the Clinical Skills Assessment Test (CSAT) of Newfoundland and Labrador, and the Clinical Assessment for Practice Program (CAPP) of Nova Scotia.
I was fortunate to obtain 6 months of training with JB, a psychiatrist who is very experienced in teaching communication skills. On observing my interview style, he said I had “a machine-gun approach”—a striking metaphor. He made me realize that I showed little empathy toward the patient and had developed the bad habit of firing away questions in order to score as many points as possible in the limited time allotted in exam settings.
JB taught me how to do patient-centred interviewing. He taught me the feelings, ideas, function, and expectations (FIFE) model.[6] The FIFE model, which was developed at the University of Western Ontario, explores the patient’s emotions, his or her ideas on what caused the problem, the effects of the illness on his or her functioning and relationships, and his or her expectations for the future and from medical care. JB also used analogies that I found wonderfully easy to understand. I remember him describing the interview as a dance in which sometimes the physician leads and sometimes the patient leads.
Outcome
In health care today, we are very aware of measurements and outcome. The outcome for me after training was measured by my success in my examinations, and it was good. Using the skills that I learned, I was able to pass every clinical exam that I tackled. I passed my Licentiate exam (LMCC), the IMGBC OSCE 2008 (which had tougher odds than when I took it in 2007), the CSAT of Newfoundland and Labrador, and the CAPP of Nova Scotia.
Today I have moved on from the “machine-gun approach” to the FIFE interview format. Simulated patients have made many positive comments about my performance in the exam setting: “He makes an excellent introduction and makes it very clear that I would be cared for”; “He is very skillful… I would be happy to have him as a doctor”; “He has a professional and confident demeanor, and is not flustered easily”; “His empathetic comments are disarming”; “He established rapport through the use of age-appropriate language and questions, effective listening skills and he is calming, friendly and open” (OSCE results letters from Drs R. Maudsley, K.E. Burke, and M.T. Chiasson, 20 August 2008). Indeed, patients’ satisfaction was high in all the clinical exams I went through and I succeeded in meeting critical elements in 100% of the cases presented to me.
Importance of training
Having seen what can happen when an experienced trainer helps a trainee acquire a new and deep awareness of patient-centred interviewing, we decided to follow up on the progress of other international medical graduates who did not pass the IMGBC OSCE 2007. At the outset, we knew that many IMGs were doing parts of the patient-centred interview intuitively and haphazardly.
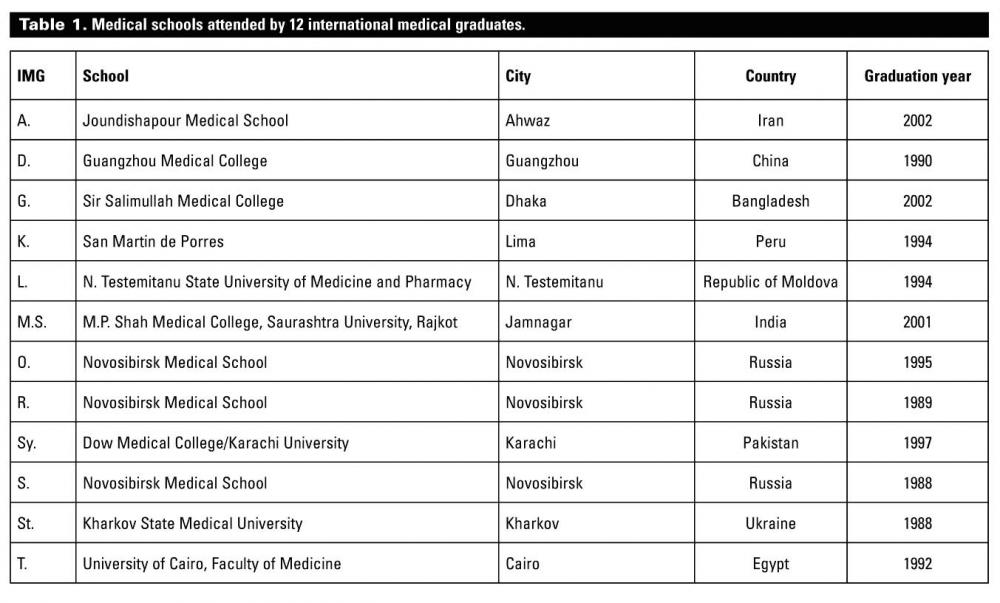
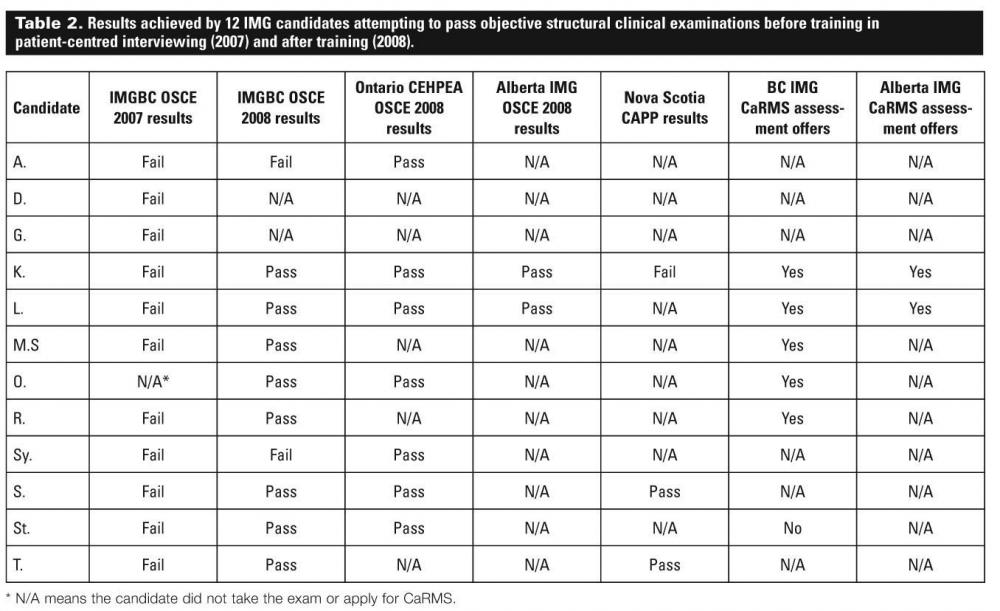
We examined data from 12 IMGs (including myself—TK) who attended 10 different foreign medical schools on four continents (Table 1). All subjects reported that they had not received any formal patient-centred interview training at their respective medical schools and 11 candidates (one did not take the exam) failed the IMGBC OSCE 2007 (Table 2). However, after I received formal training from JB and discussed my new skills with my 11 IMG colleagues, the mere incidental transfer of knowledge led to amazing results. Out of 10 candidates who repeated the IMGBC OSCE in 2008, 8 received passing scores. All 7 candidates who took the equivalent examinations offered by the Centre for the Evaluation of Health Professionals Educated Abroad (CEHPEA) in Ontario passed, 2 candidates who took the Alberta examination also passed, and 2 out of 3 candidates who took the Nova Scotia CAPP assessment passed. Subsequently, 5 of the 6 IMGs who took the BC CaRMS assessment were offered residencies and the 2 candidates who took the Alberta CaRMS assessment were offered residencies.
{kind=link}
{kind=link}
Conclusions
Ours is a small but striking audit. Certainly, both measurement and selection biases exist. In order to better measure the impact of communication skills training in IMGs, a larger sample would have to be studied, and the subjects of the study would need to follow the same training curriculum and take exactly the same assessment exams. Further study is merited considering the potential benefits.
First, focused training could help IMGs prepare better for costly examinations. IMGs face a heavy financial burden in taking examinations. For example, the CAPP of Nova Scotia costs $6500 and historically only 13% to 19% of its applicants have passed. The CSAT of Newfoundland costs around $4000 and the training involved typically costs around $13 000 before a licence is issued.
Second, training could prepare IMGs for the realities of practice. Medical practitioners conduct between 120 000 and 140 000 interviews in an average 40-year medical career.[1] As IMGs will also conduct thousands of interviews once in practice, it is imperative that they obtain formal training in interviewing skills.
Furthermore, if we are to be serious about retraining IMGs, then it might be worthwhile to learn more about the training in communication skills that they receive in their home countries, and then use that information to design an integrated educational program that would enhance those skills. This could benefit even those who are long-term practising clinicians, as was my case.
Government and provincial colleges of physicians and surgeons would do well to recognize these specific needs of IMGs. The training of IMGs should focus more on communication and interviewing skills, including emphasis on cross-cultural and language challenges. Only then will Alice James’s soul rest in peace.
Competing interests
None declared.
Acknowledgments
We are grateful for the assiduous moral support of both Dr Sheldon Zipursky (head of department) and Dr Harry Karlinsky (education director) of the Department of Psychiatry at Richmond Hospital, British Columbia.
___________________________________________________________________
The College of Physicians and Surgeons of British Columbia responds
The College is supportive of efforts to improve success on the screening examinations required by the various international medical graduate programs in Canada. For some years the College has licensed IMGs on the educational register as clinical trainees, thus providing them an opportunity to acculturate to the Canadian medical system in hospitals and physicians’ offices where there is an opportunity to learn the intricacies of Canadian medicine and hone communication skills. Dr Khalil and Dr Bhopal’s article suggests that even with such opportunities IMGs often lack training in communication skills and knowledge of the OSCE patient-centred format to be successful in those examinations. The College encourages the University of British Columbia and the provincial government to examine whether a communication training program could be made available to IMGs. This would unequivocally benefit both IMGs attempting to enter a residency program, as well as IMGs licensed to practise in British Columbia who are required to complete Canadian examinations such as the Medical College of Canada Qualifying Examination Part 2.
—Elliott J. Phillips, MD
Deputy Registrar
College of Physicians and Surgeons of British Columbia
___________________________________________________________________
References
1. James A. Edel L (ed). The Diary of Alice James. Boston: Northeastern University Press; 1999.
2. Peabody FW. Landmark article March 19, 1927: The care of the patient. JAMA 1984;252:813-818. PubMed Abstract
3. Cole S, Bird J. The medical interview: The three-function approach. 2nd ed. St. Louis: Mosby Publishing; 2000.
4. Bates J. Medical school expansion in BC. BCMJ 2008;50:368-370.
5. Webber E, Rungta K, Sivertz K. Expansion of postgraduate medical education. BCMJ 2008;50:384-387.
6. Weston W, Brown BB, Stewart MA. Patient-centred interviewing. Part 1: Understanding patients’ experiences. Can Fam Physician. 1989;35:147-151.
Dr Khalil is an international medical graduate from Egypt. He graduated from Cairo University in 1992 and is currently practising as a family physician in Halifax, Nova Scotia, under the Clinician Assessment for Practice Program. Dr Bhopal is an international medical graduate from Glasgow University. He graduated in 1974 and has been practising in British Columbia since 1978. Currently, he practises in Richmond, BC, and is also a clinical assistant professor in the Department of Psychiatry at the University of British Columbia.