Management of cancer pain with opioids
Issue: BCMJ,
vol. 63 , No. 9 , November 2021 ,
Pages 372-376 Clinical Articles
ABSTRACT: Opioid-based analgesia is the most appropriate primary approach for treatment of moderate to severe cancer pain. “Weak” opioids (i.e., those that have a ceiling effect), such as codeine, tramadol, and buprenorphine, are more potent and more predictably effective than non-opioids but have significant limitations. “Strong” opioids include morphine, hydromorphone, oxycodone, fentanyl, and methadone. Morphine is the recommended first-line opioid for cancer pain but not when there is renal impairment or in frail older patients. When compared to morphine, hydromorphone has less potential for toxicity from metabolites, but comes in fewer strengths and forms. Oxycodone is useful when morphine or hydromorphone are not well tolerated; however, it can cause agitation. Transdermal fentanyl is a second- or third-line opioid that can have an important role when the oral route is compromised or when constipation is particularly troublesome. Methadone is more complex to use than other opioids, but it may be better tolerated and more effective. It plays a particularly important part in renal failure because it is not dialysed out and has no active metabolites. Methadone can also provide excellent analgesia without neurotoxicity, and has shown good effects in treating neuropathic pain. It is also the only relatively long-lasting opioid that can be easily swallowed in liquid form or put through a gastrostomy tube. Buprenorphine can be used where respiratory depression is a significant concern, such as in sleep apnea or chronic obstructive pulmonary disease with carbon dioxide retention. The risk of developing an opioid use disorder from opioid therapy is not a concern for most cancer patients, but safe prescribing practices should be followed.
Non-opioid analgesics are frequently ineffective or only mildly effective for cancer pain and can cause potentially serious side effects. Lidocaine and ketamine infusions can provide good pain relief for those with severe cancer pain that is not adequately managed with opioid treatments. A variety of interventional procedures, such as anesthetic interventions, neurosurgical procedures, and interventional radiological procedures, can be dramatically beneficial when medications are not effective or not tolerated. Minimally invasive palliative procedures can provide excellent relief, even in very frail patients.
A review of cancer pain management methods suggests that the use of opioid-based analgesia is the most appropriate primary approach to treating moderate to severe cancer pain.
Approach to managing cancer pain
Over the past 2 decades, cancer has been the leading cause of death in Canada, at just over 80 000 deaths per year in 2019.[1] Heart disease trailed by a large margin, at 52 541. The eight other leading causes of death were (in decreasing order) accidents, cerebrovascular disease, chronic lower respiratory diseases, diabetes, influenza/pneumonia, Alzheimer disease, suicide, and kidney disease. In addition to cancer, stroke, diabetes, and renal failure are also associated with significant painful sequelae. This article focuses on cancer pain and the appropriate use of opioids, but the principles of cancer pain management apply to people living with many other serious chronic illnesses.[2]
Cancer is overwhelmingly the most common reason for requesting medical assistance in dying, primarily because of fear of loss of function (usually due to pain) that leads to loss of autonomy and the ability do the things that people used to enjoy, and because of fear of a painful death.[3] Poor pain management or stigmatization about the need for opioid analgesia contributes to those fears. Dignity-conserving care is integrally linked to provision of good pain management.[4]
Cancer pain is not a single entity. The choices of treatments that are most appropriate for any individual will depend on multiple factors, both disease related and host related. Pain can be caused by cancer itself, or by cancer treatments such as surgery, radiotherapy, and systemic therapies (chemotherapy, hormone therapy, targeted therapy, and immune therapy). The complications of immunosuppression can also be painful, particularly from shingles and postherpetic neuralgia. Pain in the survivorship context is becoming more and more common as new oncology treatments prolong survival, and some successful palliative oncology treatments make cancer pain management closer to the chronic disease model.
Most cancer pain can be controlled, but in reality many patients live with inadequate pain management because of lack of knowledge, reluctance to use easily available therapies, or difficulty accessing therapies due to financial, geographic, or system-related barriers. Fear of regulatory oversight has become particularly widespread in recent years, despite the College of Physicians and Surgeons of BC publishing clear guidance that opioid prescribing is appropriate for cancer pain and in palliative care, and that to not prescribe opioids when medically appropriate is just as unacceptable as prescribing opioids when not indicated.[5,6]
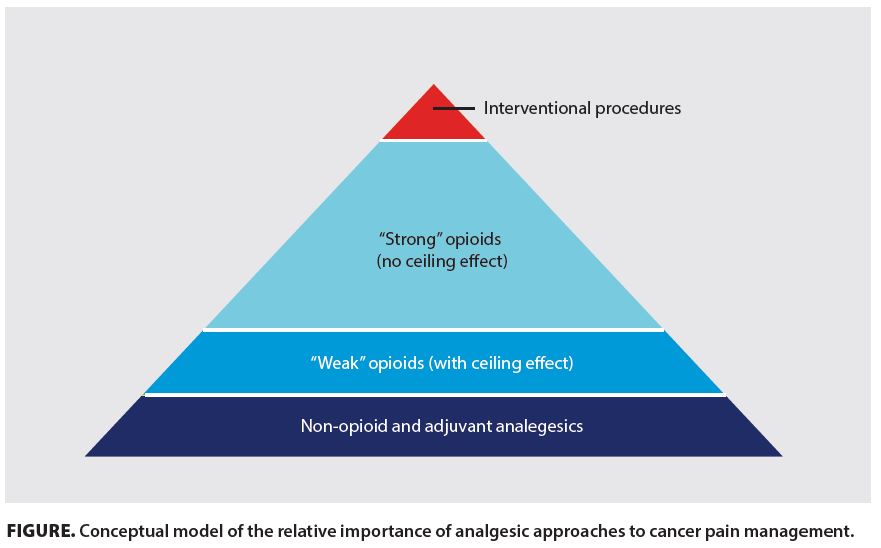
The conceptual model shown in the Figure, derived from the World Health Organization analgesic ladder, describes the relative importance of analgesic approaches to cancer pain management. Note that this is not intended to be a stepwise approach to care; starting with low doses of a Step 3 (“strong”) opioid analgesic may be the best approach when pain is already moderate or severe [Figure].
Non-opioids and adjuvant analgesics
Simple analgesics alone, such as acetaminophen and nonsteroidal anti-inflammatory drugs, may be helpful in early-stage cancer in which pain may be mild or intermittent, and adjuvant analgesics, such as tricyclics or gabapentin/pregabalin, may offer some relief when there is a neuropathic component to the pain. Tricyclics can be tried in low doses (usually 10 mg/day with titration at weekly intervals to a maximum of 50 mg), preferably with nortriptyline if some night sedation is also desired, or desipramine/imipramine if sedation is to be avoided. Amitriptyline has more side effects than other tricyclics and is no better an analgesic for neuropathic pain. Medical cannabis would be included in this part of the model, but discussion of this is beyond the scope of this article. Non-opioid analgesics, however, are frequently ineffective or only mildly effective and can cause potentially serious side effects. They should be approached as n-of-1 trials, in which only one thing is changed at a time, the effects are carefully assessed, and the analgesic discontinued if it is not helpful.
“Weak” opioid options
“Weak” or World Health Organization (WHO) analgesic ladder Step 2 opioids are more potent and more predictably effective than non-opioids but have significant limitations. Drugs in this step, by definition, have a ceiling effect. Codeine and tramadol require activation by hepatic enzyme pathways that have genetically determined and variable rate-limiting capacity. Some combination preparations contain an opioid that does not require activation but may be deemed Step 2 because of the toxicity of the attached non-opioid, usually acetaminophen; for example, acetaminophen/codeine or acetaminophen/oxycodone combinations (Tylenol #3 or Percocet). Buprenorphine is slightly different because its ceiling effect comes from mixed agonist/antagonist activity at the opioid receptor level; this is discussed in more detail below.
It should be noted that the WHO analgesic ladder is a classification system for analgesics; it is not a clinical practice guideline. Step 2 analgesics have a very small role to play in the management of chronic cancer pain but may be appropriate when pain is present only intermittently or is expected to improve rapidly; for example, in postsurgical/procedural pain or short-lived pain during certain activities. Most Step 2 opioids have a short half-life and require 4- or 6-hourly dosing. Converting from a Step 2 opioid preparation to a Step 3 opioid carries a risk of overdosing or underdosing in the transition because of the unpredictability of equianalgesic dose ratios inherent in the genetic variability of the enzymatic activation function between individuals. Most cancer pain has at least some element of continuous pain, with intermittent exacerbations. Step 3 opioids are indicated and can be started in low doses without having used a Step 2 opioid beforehand. Step 4 includes palliative procedures such as nerve blocks, cementoplasty, neuraxial infusions, and neurolytic procedures, but a small minority of cancer pain patients who could benefit from them currently receive these treatments.[7]
It is important to identify whether there is a neuropathic component to cancer pain because this can influence the choice of treatments. It is also important to identify the presence of an incident component to the pain—i.e., pain that starts abruptly and lasts only a short while—because this will require the use of short-acting rather than (or in addition to) sustained-release opioids.
“Strong” opioid options
Morphine. The recommended first-line opioid for cancer pain is morphine, which is available in multiple formulations: immediate-release oral tablets or solution, sustained-release tablets or capsules (12 or 24 h), and parenteral solutions. Morphine is not recommended when there is renal impairment or in frail older patients because of the potential for accumulation of metabolites. An appropriate starting dose for continuous cancer pain in a patient who has not had any prior opioid treatment (i.e., opioid-naive) would be morphine 5.0 mg every 4 hours regularly plus 2.5 mg every hour as needed, with transition to appropriate sustained-release dosing replacing the every-4-hour regular dosing as soon as requirements are known. Initiation with 10 mg sustained release every 12 hours is equally reasonable and may be a better choice for those at home, and may have a better chance of compliance.
Hydromorphone. Hydromorphone is a widely used alternative to morphine and has less potential for toxicity from metabolites, but it comes in fewer strengths and forms, and the sustained-release capsules (12 or 24 h) require special authority or a specific plan for PharmaCare coverage (e.g., BC Palliative Care Benefits [Plan P]). It has approximately 5 times the potency of morphine (1 mg hydromorphone is equivalent to 5 mg morphine), though this can vary between individuals. The injectable form is more soluble than morphine when high concentrations are required. Hydromorphone is a good first choice opioid if morphine is contraindicated, and it is appropriate to switch to it if a patient is experiencing side effects from morphine. Awareness of the PharmaCare coverage issues for the sustained release capsules is, however, an important consideration if morphine is bypassed.
Oxycodone. Oxycodone is also a useful oral opioid, particularly when morphine or hydromorphone are not well tolerated. It is slightly more potent than morphine: 5.0 mg oxycodone is approximately equivalent to 7.5 mg morphine. Sustained-release oxycodone is available in a matrix tablet form (generic OxyContin) and in an abuse-deterrent gel tablet form (OxyNEO), which becomes sticky when wet and requires good swallowing function. Oxycodone can sometimes cause agitation, despite effective analgesia. It is also not available in injectable form in Canada. Cost and PharmaCare coverage can be a concern if a patient is not eligible for BC Palliative Care Benefits.
Fentanyl. Transdermal fentanyl is a second- or third-line opioid, which can have an important role when the oral route is compromised or when constipation is particularly troublesome. If switching to fentanyl, it is important to use a current conversion chart[8] to select an appropriate dose, and to consider a stepped transition because of marked interindividual variability in pain responsiveness to different opioids and in absorption and metabolism. Equivalent doses may differ substantially in any one individual from those expected from consulting a chart. It is also important to have an overlap of at least 12 h between the oral and transdermal preparations because of the delay in reaching stable blood levels of fentanyl once a patch is applied. Cost and PharmaCare coverage may be a concern if a patient is not eligible for BC Palliative Care Benefits.
Methadone. Methadone has a special role in cancer pain management. It is more complex to use than other opioids, so it is rarely considered a first-line opioid; however, in many patients it may be better tolerated and more effective than other opioids.[9,10] A short (1 h), free CME-accredited online module, Methadone4Pain.ca, is presented by Canadian Virtual Hospice and provides clear instructions on how to use methadone safely in the palliative care context.[11] The College of Physicians and Surgeons of BC website also has a handbook on prescribing methadone for analgesia.[12]
In BC, methadone for pain is prescribed on a regular controlled prescription pad. No special authorization is required. Methadone is available as a 10 mg/mL solution and in tablets, which are covered by the BC Palliative Care Benefits Program. Lower strengths require compounding and could cause confusion with dosing. Small volumes for analgesic doses need to be carefully measured with a 1 mL syringe, so tablets are preferable. Methadone has a long half-life and is stored in body fat, so a “start low, go slow” approach of making dose increases no more frequently than every 3 days should always be taken, if possible, and ideally every 5 to 7 days if the clinical situation allows. Methadone can be added to another opioid in this fashion in an adjuvant role, with weekly review and adjustment. Fast starts are more complex because of unpredictable potency; thus, stepped conversions from other opioids, as described in the Methadone4Pain module, should be practised in all but specialist palliative care settings where the close supervision necessary for a “stop and go” or rapid stepped switch is available. In high doses (> 120 mg/day), methadone can cause prolongation of the QT interval. Providing that the goals of care are appropriate, an ECG should be checked if the dose reaches that threshold or if the patient is at risk of QT prolongation due to a concurrent condition, inherited predisposition, or concurrent treatment with other potentially QT-prolonging drugs. Methadone also has more interactions with non-opioid drugs; the commonly encountered ones to be aware of are ciprofloxacin and fluconazole. Methadone can also interact with grapefruit.
Methadone plays a particularly important role in renal failure because it is not dialysed out and has no active metabolites. Similarly, where delirium has occurred with other opioids, a switch to methadone can allow for excellent analgesia without neurotoxicity. Though yet to be proven in randomized controlled trials, many experienced prescribers see particularly good effects from methadone in treating neuropathic pain. Methadone also has the advantage of being the only relatively long-lasting opioid that can be easily swallowed in liquid form or put through a gastrostomy tube. This can allow families relief from 4-hourly medication administration when transdermal fentanyl may not be effective or appropriate; for example, in children who need finer tuning of dosing than can be achieved with the limited choice of patch strengths, or in adults with cognitive or behavioral issues who might peel the patches off. Methadone also has a niche in the treatment of patients who require long-term opioid therapy because it has less of a propensity to cause tolerance and dose escalation than other opioids. If methadone is started by a specialist palliative care program or oncologist, it is important for family doctors and nurse practitioners to take over prescribing when patients are stable. This allows the specialist services to maintain capacity to see new patients, ensures closer supervision than can be provided by a specialist clinic, helps avoid drug interactions, and most importantly, allows patients who are approaching end of life to be well cared for in the community. Methadone oral solution is well absorbed rectally and sublingually/buccally for those who are unable to swallow. Methadone liquid is inexpensive and is covered by PharmaCare; methadone tablets are covered by BC Palliative Care Benefits. Special authority for 1 mg/mL compounding can be applied for, and is usually more appropriate for analgesia patients than the 10 mg/mL solution.
Other opioids. Other opioids that have a limited but important role in the management of cancer pain include buprenorphine and sufentanil. Oral buprenorphine combined with naloxone (Suboxone) is well known for its usefulness in the management of opioid use disorders, but buprenorphine also has a role in chronic pain management where respiratory depression is a significant concern; for example, in sleep apnea or chronic obstructive pulmonary disease with carbon dioxide retention. It can also be an excellent choice as an alternative to methadone for pain, but care has to be taken with transition from a full agonist opioid to buprenorphine because of the agonist–antagonist effect it has on the opioid receptors, which could theoretically trigger a partial withdrawal reaction. In practice, this does not seem to be a problem.[13] Buprenorphine is available as a transdermal patch that lasts for 1 week, and the lowest strength is 5 mcg/h, which is equivalent to less than 30 mg oral morphine per day (or approximately six Tylenol #3/day in a normal metabolizer).
Non-opioid analgesics
Lidocaine and ketamine infusions can provide good pain relief for those with severe cancer pain that is not adequately managed with the WHO analgesic ladder approach, and while they are generally initiated in specialist settings, they may be required over extended periods in settings where there is no access to pain specialists. For this small but important group of patients, it is important that other services are comfortable taking over the delivery of these analgesics once the patient is stabilized and the appropriate treatment protocol has been determined. Unfounded fears about arrhythmias have been a significant barrier to access to lidocaine, which is inexpensive, effective in approximately 50% of patients, and very well tolerated providing simple safety measures are followed.[14] There is less evidence to support the use of ketamine as an analgesic, but there is sufficient clinical experience with it to suggest that in low doses it may be a valuable addition to the treatment options for those unfortunate cancer patients with the most difficult pain syndromes.[15]
Opioid side effects
Morphine, hydromorphone, and oxycodone all have a similar propensity to cause constipation; thus, a preventive stepped laxative schedule (bowel protocol) should always be initiated at the same time as commencing an oral opioid. A good example is available on the BC Cancer website at www.bccancer.bc.ca/health-info/coping-with-cancer/managing-symptoms-side-effects/constipation-caused-by-your-medications. Fentanyl and methadone have fewer effects on bowel motility, but a bowel protocol is usually still required. Sennosides and osmotic laxatives are equally effective, but patients often prefer sennosides because of the ease of swallowing, low cost, and ease of dose adjustment.[16] Lactulose tends to generate gas, leading to bloating, and polyethylene glycol requires significant volumes of fluid, which may be difficult for some cancer patients, especially when approaching end of life. Polyethylene glycol is also not covered by BC Palliative Care Benefits.
All opioids can cause respiratory depression in the acute context, but patients rapidly develop tolerance to the respiratory depressant effect of opioids with continuous exposure, and low dose opioids can be used safely in patients with breathlessness from severe lung disease[17] or heart failure.[18] All opioids are relatively contraindicated in patients with severe sleep apnea, but buprenorphine is less likely than full opioid receptor agonists to suppress respiration when an opioid is absolutely required.[19]
Palliative procedures
Treatment of the underlying cause of pain is always the preferred approach to cancer pain management, alongside pharmacological management. Procedures have been included as a fourth step in a modified WHO analgesic ladder, and include anesthetic interventions, neurosurgical procedures, and interventional radiological procedures. Minimally invasive palliative procedures can provide excellent relief, even in very frail patients [Table].
If a one-time (repeatable) procedure is not effective or does not last long enough, implanted devices can be used; they are more invasive but still well tolerated. Intrathecal infusions can be maintained percutaneously in hospitalized patients for short periods, but fully implanted pump systems are preferred if the patient is well enough to tolerate the insertion procedure because they can be maintained at home, and patients can bathe and move independently of an external pump and tubing. For those with severe pain in the survivorship context, an implanted spinal cord stimulator can be used; it requires much less maintenance than an implanted intrathecal pump.
These Step 4 treatments are required in only a minority of cancer patients, but all patients should have access to them if appropriate pharmacological therapy does not provide satisfactory relief.[20] Awareness of the existence of these treatments is key to being able to reassure patients that their pain is treatable. If an effective procedure or treatment is available, pain still needs to be managed while waiting to set up the treatment, or for it to take effect, by using the same techniques as for long-term analgesic management.
Opioid-unresponsive pain
The analgesics and palliative procedures described above can provide good pain relief for most cancer patients, but it must not be forgotten that pain is more than just a physical experience. Existential suffering without peripheral nociceptive input can be experienced as pain, and the experience of physical pain can be magnified by existential suffering. This kind of “total pain” will not be relieved by traditional analgesics. Meticulous assessment and management of social, psychological, or spiritual factors is essential in providing effective patient-centred care for pain from serious illnesses such as cancer, and a multidisciplinary team is required to ensure that all facets of patient suffering are recognized and addressed.
Summary
Opioid-based analgesia is the most appropriate primary approach for treatment of moderate to severe cancer pain. Non-opioid medications for cancer pain all have significant limitations, which restrict their effectiveness and safety. Nonpharmacological therapies for cancer pain can be difficult to access and should be used concurrently with opioid pharmacotherapy.
The risk of developing an opioid use disorder from opioid therapy for cancer pain is low, and for most cancer patients is not a concern. However, safe prescribing practices should be followed.
Competing interests
None declared.
This article has been peer reviewed.
References
1. Statistics Canada. Leading causes of death, total population, by age group. Accessed 28 February 2021. www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401.
2. Yang J, Bauer BA, Wahner-Roedler DL, et al. The modified WHO analgesic ladder: Is it appropriate for chronic non-cancer pain? J Pain Res 2020;13:411-417.
3. Wiebe E, Shaw J, Green S, et al. Reasons for requesting medical assistance in dying. Can Fam Physician 2018;64:674-679.
4. Chochinov. HM. Dignity-conserving care—A new model for palliative care: Helping the patient feel valued. JAMA 2002;287:2253-2260.
5. Oetter HM. Registrar’s message—new practice standards approved by the Board—now in effect. College Connector 2018;6. Accessed 17 September 2021. www.cpsbc.ca/news/publications/college-connector/volume-6-no-3-may-jun-2018-8.
6. College of Physicians and Surgeons of British Columbia. Practice standard: Safe prescribing of opioids and sedatives. Accessed 17 September 2021. www.cpsbc.ca/files/pdf/PSG-Safe-Prescribing.pdf.
7. Miguel R. Interventional treatment of cancer pain: The fourth step in the World Health Organization analgesic ladder? Cancer Control 2000;7:149-156.
8. BC Guidelines. Palliative care for the patient with incurable cancer or advanced disease. Part 2: Pain and symptom management. Appendix B: Equianalgesic conversion for morphine. 2017. Accessed 28 February 2021. www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc-guidelines/palliative-pain-management.
9. Porta-Sales J, Garzón-Rodríguez C, Villavicencio-Chávez C. et al. Efficacy and safety of methadone as a second-line opioid for cancer pain in an outpatient clinic: A prospective open-label study. Oncologist 2016;21:981-987.
10. McPherson ML, Walker K, Davis M. et al. Safe and appropriate use of methadone in hospice and palliative care: Expert consensus white paper. J Pain Symptom Manage 2019;57:635-645.
11. Canadian Virtual Hospice. Methadone for pain in palliative care. Accessed 17 Sept 2021. www.methadone4pain.ca.
12. College of Physicians and Surgeons of British Columbia. Methadone for analgesia guidelines. Accessed 17 September 2021. www.cpsbc.ca/files/pdf/DP-Methadone-for-Analgesia-Guidelines.pdf.
13. Lundorff L, Sjøgren P, Hansen OB, et al. Switching from high doses of pure μ-opioid agonists to transdermal buprenorphine in patients with cancer: A feasibility study. J Opioid Manag 2013:9:255-262.
14. Lee JT, Sanderson CR, Xuan W, Agar M. Lidocaine for cancer pain in adults: A systematic review and meta-analysis. J Palliat Med 2019;22:326-334.
15. Bell RF, Eccleston C, Kalso EA. Ketamine as an adjuvant to opioids for cancer pain. Cochrane Database Syst Rev 2012. doi: 10.1002/14651858.CD003351.pub2.
16. Hawley P, MacKenzie H, Gobbo M. PEG vs. sennosides for opioid-induced constipation in cancer care. Support Care Cancer 2020;28:1775-1782.
17. Johnson MJ, Currow DC. Opioids for breathlessness: A narrative review. BMJ Support Palliat Care 2020;10:287-295.
18. Dawson NL, Roth V, Hodge DO, et al. Opioid use in patients with congestive heart failure. Pain Med 2018;19:485-490.
19. Dahan A, Yassen A, Romberg R, et al. Buprenorphine induces ceiling in respiratory depression but not in analgesia. Br J Anaesth 2006;96:627-632.
20. Sindt JE, Brogan SE. Interventional treatments of cancer pain. Anesthesiol Clin 2016;34:317-339.
Dr Hawley is a general internist and palliative medicine subspecialist who founded the BC Cancer Pain and Symptom Management/Palliative Care (PSMPC) service in 1997. She is the provincial medical director of the program and leader of the Vancouver Centre’s PSMPC team. She is also the head of the UBC Division of Palliative Care.

{kind=link}