The implementation of a physician workload system in an academic health care setting: The Physician Activity Information System
Background: The multiple roles that academic physicians fulfill present a challenge when quantifying physician workload. How these differing roles are integrated within a specialist group at an academic health care centre has not been well documented. In 2004 an in-house system for measuring workload was implemented in the Division of Maternal Fetal Medicine at BC Women’s Hospital and Health Centre in collaboration with the Information Management/Information Technology department of the Provincial Health Services Authority.
Methods: The Physician Activity Information System (PhAIS) was developed to report on workload patterns for 15 salaried subspecialists. The system uses Microsoft Outlook to collect and code data according to 41 categories of clinical and nonclinical activities, and a middleware application to extract and analyze the data. The data are then collated and summarized on a monthly basis and submitted to the Ministry of Health and individual division members.
Results: Data collected for 3 consecutive years from 2004 to 2007 were analyzed to compare hours spent on clinical and nonclinical activities and the workloads of male and female physicians and physicians at junior, middle, and senior stages in their careers. Averaging the hours of workload as categorized by PhAIS and adjusting the workload by the number of full-time equivalents shows that the differences found are explainable by career orientation, physician seniority, and lifestyle factors.
Conclusions: PhAIS ably supports the accountability and transparency requirements of today’s health care environment and meets reporting standards at local and provincial levels. Data are now available for use when defining physician workload components in an academic health care setting.
Data gathered by workload measurement processes developed in BC provide quality and accountability measures that are valuable to employers, administrators, and individual physicians.
Quantifying the workload of an academic physician is challenging because the physician’s workload consists of so many different components. For example, as well as undertaking clinical and consulting activities, an individual physician may be an educator and an administrator. The time and resources required to obtain an accurate measurement of the physician’s workload may outweigh the advantage of tracking the activities.
Although workload measurement systems are not novel in clinical fields, the literature around the development of physician systems is sparse.[1-3] Systems have existed for over 20 years in the allied health professions because of their predominantly salaried nature and the requirement for accountability at an institutional and professional level.[4]
Physicians receive payment for their services based on many funding models, including fee-for-service, sessional, salary, and a combination of these. The ability to act as a care provider and consultant in addition to acting as an educator, researcher, and administrator is contingent upon these arrangements. These roles often overlap in the day-to-day work life of many physicians. The Division of Maternal Fetal Medicine in the Department of Obstetrics and Gynaecology at the University of British Columbia has been endeavoring to quantify the workload of its physicians for more than 5 years. The division consists of 15 salaried maternal fetal medicine specialists who provide high-risk pregnancy services at a tertiary perinatal provincial centre. Embedded in the Maternal Fetal Medicine divisional strategic plan is a documented commitment to develop and implement a workload measurement system that tracks and reflects the salaried physicians’ concurrent roles, which involve both clinical and nonclinical mandates. The division is now required at a provincial and institutional level to demonstrate accountability. The ability to track and categorize work activities by electronic means has allowed the division’s physicians to compartmentalize components of their daily activities in a way that illustrates their multiple roles. These roles and workload components have been defined as follows:
• Clinical: defined as patient-centred activities with or without the patient present. Examples include consulting with patients in person or by telephone, undertaking procedures, completing charts, and writing reports.
• Nonclinical: defined as academic activities involving education, administration, and research. Examples include teaching undergraduate students, performing research, advancing practice by establishing evidence-based guidelines, and participating in leadership activities that contribute to local, provincial, or national professional organizations.
In combination, clinical and nonclinical activities constitute the role of an academic physician. Similar components have been defined elsewhere, such as in a measurement system at Louisiana State University that calculated its faculty involvement using four parameters: teaching, research, administration, and patient care.[1]
Management information gathered by a workload measurement system provides quality and accountability measures that are highly valuable to stakeholders, employers, administrators, and individuals. For example, the largest health management organization in the United States, the Veterans Health Administration, has used physician productivity measurement models to substantiate their physicians’ clinical and nonclinical roles.[2]
The Physician Activity Information System (PhAIS) was developed in 2004 in a collaborative project involving the Division of Maternal Fetal Medicine and the Provincial Health Authority’s Information Management/Information Technology (IM/IT) department, both located at BC Women’s Hospital and Health Centre.
Division of Maternal Fetal Medicine physician workloads were measured manually starting in 1997. After several years of this, the development of a comprehensive computerized system was identified as a strategic goal. The primary objective of the project was to categorize and integrate the various work activities under the broad deliverables of clinical and nonclinical activities into a systematic monthly reporting system. Such a system would meet local and provincial reporting requirements and serve as a meaningful management tool for resource and productivity purposes.
The Information Management/Information Technology department assisted the division in identifying available application products that could fulfill the objectives of the project. Products were evaluated based on cost, complexity, hardware requirements, software requirements, training needs, system support, and application architecture. Various products were available to measure workload but were found to be a poor fit with the division’s environment. Eventually a product was chosen and modified to meet the division’s requirements.
Infrastructure development and setup
After Microsoft Outlook was identified as an application commonly used by the division’s subspecialty physicians to schedule their activities, an MS Outlook feature called “Categories” was customized and used to move forward with the PhAIS project. Through discussions and fine-tuning, the division defined a set of categories to use when capturing physician activities.
Initially, the division purchased personal digital assistants (PDAs) for the physicians to schedule and categorize their own workloads on a daily basis. However, over time the PDAs proved less useful than originally anticipated because of hardware and software issues and the need for frequent technical support. Furthermore, real-time data entry became a cumbersome and time-consuming activity for the physicians. As a consequence, categorizing of work activity became the responsibility of the administrative staff, who completed the task either at the end of the day or the end of the week using a desktop application. Considerable training time was invested early on to help administrative staff capture work activities accurately, and an open dialogue among the administrative staff ensured ongoing consistency. Using MS Outlook enabled the division and the IM/IT department to reduce infrastructure costs. Instead of investing time and resources in a completely new system, the division focused on training staff to work with the categories in a program they were already using.
Database design and management
The next step in the project involved creating a database to capture the activity categories from MS Outlook so that customized reports could be developed to track the workload statistics for each physician and the division as a whole. In order to extract data in a cost-effective manner, a middleware application called Global Calendar DB Service was purchased from a Danish company (www.completesoftware.dk). Extensive testing was undertaken and then the data extracted were compared with the workload statistics captured manually by the division schedule. Initially, major discrepancies needed to be rectified by providing additional training on categorizing activites for the administrative staff and folding some categories into broader category descriptions. After a series of adjustments, the extracted data were of the same calibre and reliability as the data captured manually by the division personnel.
After a 1-year trial, the database was amended substantially to capture a manageable 41 categories of clinical and nonclinical work (Table) rather than the original 100 categories. Streamlining the database reduced confusion and promoted standardization of categories when early coding work showed that the greater the number of categories, the greater the tendency for individuals to code inconsistently. Early experience also determined that entry and coding of activities were best done by the administrative staff members who managed the physicians’ calendars. Multiple working sessions were held with the administrative staff to define the workload dimensions and to standardize the approach to coding. A user group was formed and led by a key administrative member. A training manual was also developed to assist with the interpretation of the coding procedures and provide orientation for new administrative staff.
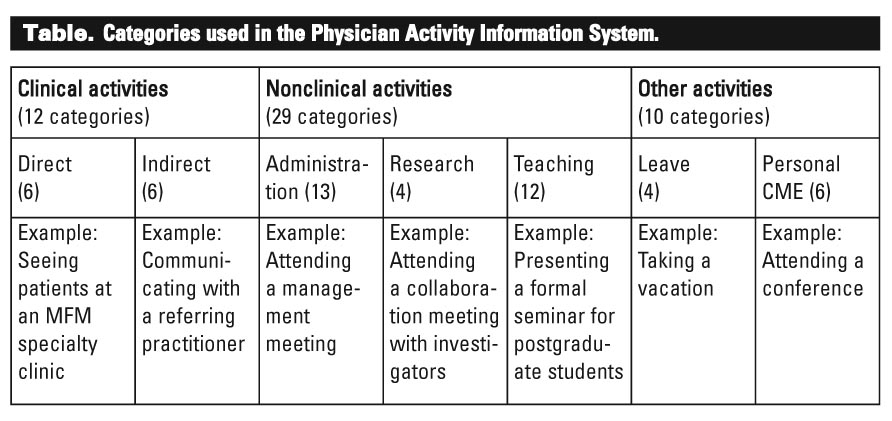{kind=link}
Today the user group continues to embrace the utility of PhAIS and an ongoing dialogue occurs to ensure consensus in categorizing activities. The lead user is also responsible for extracting and reporting the data, which is collated and summarized on a monthly basis and submitted to the Ministry of Health and individual MFM division members.
Data were collected, analyzed, and reported for 3 consecutive years from 2004 to 2007.
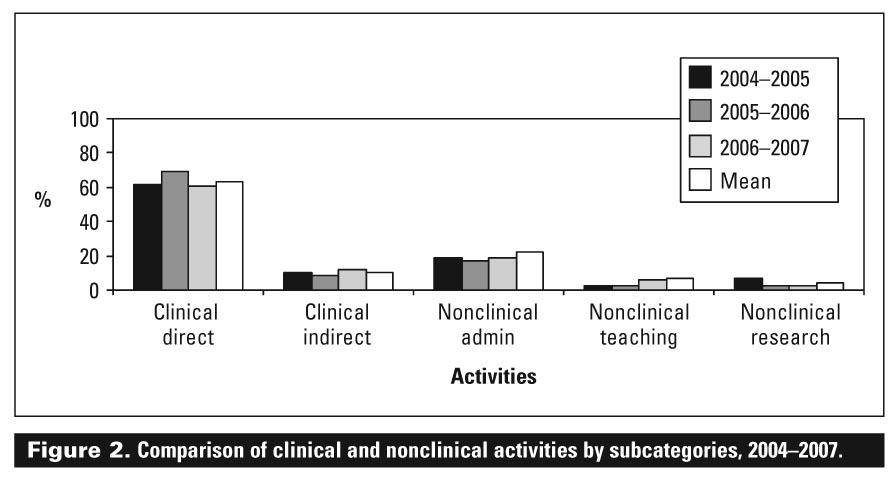
The data in [Figure 1] show that 70% to 75% of a Division of Maternal Fetal Medicine physician’s work was clinically oriented and 25% to 30% was nonclinical in each year and when averaged over the 3-year period. There is a slight variation in the comparisons year to year, but overall the average is consistent with the annual split between clinical and nonclinical work. The data in [Figure 2] show that an academic physicians’ total workload breaks down as follows:
{kind=link}
• 60% to 70% of clinical work occurs with the patient present and is considered direct patient care.
• 10% to 15% of clinical work is related to the total care of the patient (e.g., chart and report writing) and is considered indirect patient care.
• 20% of nonclinical work is administration.
• Less than 10% of nonclinical work is either research or teaching.
It is important to note that the teaching and research categories may not accurately represent the time spent on these activities, since administrative activities connected with research and teaching have been recorded under administration.
[Figure 3] compares the average hours worked by male and female physicians and shows that females spent more hours on clinical and nonclinical activities and took more time for continuing medical education and leave unrelated to CME. This can be attributed to the fact that there are more females than males in this physician group, something that can be adjusted for using the number of full-time equivalents, or FTEs (workload measure), for each physician.
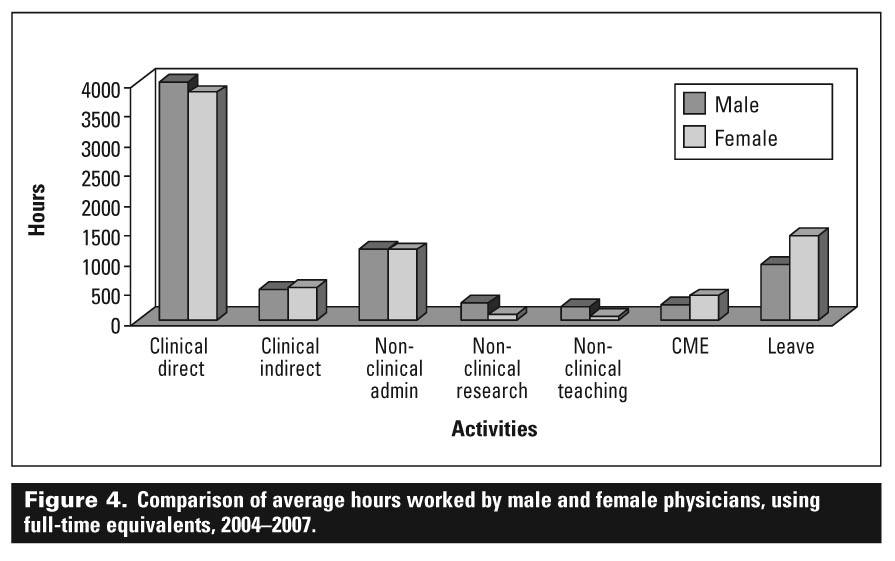
When data are adjusted for FTEs in [Figure 4], male physicians spent more time on direct patient contact, research, and teaching, while female physicians spent more time on indirect clinical activities such as report writing, CME, and leave. This difference can be attributed to lifestyle factors and maternity leaves that occurred throughout the period of data collection. Within the administration category, there was no significant difference between male and female physicians. As with [Figure 3], it is important to remember that the data shown here are not totally representative, since administrative activities for teaching and research are recorded under administration.
{kind=link}
The data in [Figure 5] show that junior staff with less than 5 years’ experience spent more time in overall clinical activities, CME, and on leave. Junior staff also spent less time on nonclinical activities such as research and administration. Physicians in their mid-career cycle (6 to 10 years) spent more time on indirect clinical, administration, and research activities, while senior staff (over 10 years) spent more time on administration and less on clinical activities.
{kind=link}
When data related to seniority are adjusted for full-time equivalents in [Figure 6], the junior physicians spent more time on total clinical activities than both the mid-career and senior physicians, whereas the senior physicians spent more time on total nonclinical activities than both the junior and mid-career physicians. The mid-career physicians’ workload categories fall between the junior and senior physicians in both the clinical and nonclinical totals. The junior physicians undertook more CME activities and were away on leave more than physicians in the other two groups. Both [Figure 4] and [Figure 6] show that more leave was taken by females and that maternity leave was common for junior female physicians during the 3 years of data collection.
{kind=link}
The data collected provide a workload profile for an academic physician by comparing work activities within a total workload, and by considering work activities according to physician gender and age.
The data also demonstrate that there are differences in workload between academic physicians by gender and age. It has been shown by collecting and averaging the hours of workload as categorized by PhAIS and adjusting the workload by the number of full-time equivalents (workload measure) that these differences are explainable by career orientation, physician seniority, and lifestyle factors.
The data may not be totally representative regarding all nonclinical activities, particularly research and teaching. These activities may be understated because of underreporting of clinical research, which is often performed outside of the usual workday or on weekends, and by the recording of administrative activities related to research and teaching under administration. Future work with PhAIS will focus on capturing all work-related activities.
Physician work is complex and the reliability of data collection depends on diligent and real-time data entry. The success of PhAIS is largely due to the infrastructure now in place and the division’s commitment to the model and engagement in the process. The time and effort invested in the development of the database, the training of administrative staff members, and the monthly monitoring of the data have been substantial. The entire process of entering activities into the electronic calendar, coding, collating, reporting, and analyzing has been successful because of the culture of accountability within the division. Notably, the PhAIS system is a process-oriented tool and the work activities do not translate into outcome information. For example, specific activities within the broad category of research, such as collaborating or writing, do not necessarily equate to the number of papers produced or number of grants secured. The 41 specific clinical and nonclinical tasks in the database are not value-specific or weighted and thus cannot be used as measures of quantitative or qualitative productivity as other systems have done.[1-3] That being said, PhAIS has been implemented in the Division of Maternal Fetal Medicine.
In the Division of Maternal Fetal Medicine PhAIS has provided a better understanding of workload within the same specialty and for individual members with varying backgrounds and at different stages of career development. Monthly reporting of PhAIS data to individual physicians has also validated physician models such as clinician-educator and clinician-leader. Recently, PhAIS data have also been used for reporting teaching hours as required by UBC for both clinical and full-time faculty. From a practical perspective, the data have also been used to substantiate and report the full-time equivalent components for the division members at an institutional and provincial level.
In summary, the Division of Maternal Fetal Medicine at BC Women’s Hospital has demonstrated the ability to develop, implement, and evaluate an electronic workload reporting system. PhAIS tracks and categorizes work activities into clinical and nonclinical activities and electronically collates these measures into various reports determined by the user. In turn, these data are used for various reporting purposes, and strategic planning activities within the health care centre and university department. This system was a result of dedicated focus and energy from the physicians and administrative team in the division and the Department of Obstetrics and Gynaecology at the University of British Columbia.
Acknowledgments
We would like to thank Dr Deborah Money for assistance in maintaining the momentum in this project and Ms Neda Amiri and Ms Marie Rivard for their assistance in entering and summarizing the data for analysis.
Competing interests
None declared.
References
1. Hilton C, Fisher W Jr, Lopez A, et al. A relative-value-based system for calculating faculty productivity in teaching, research, administration, and patient care. Acad Med 1997;72:787-793.
2. Department of Health and Community Services/Rehabilitation Services Plan Working Group #2. Workload measurement for audiology, occupational therapy, physiotherapy and speech language pathology in institutional and community settings. May 1996. www.gnb.ca/0383/pdflibrary-e/WMS_E.pdf (accessed 1 October 2008).
3. Fairchild DG, Benjamin EM, Gifford DR, et al. Physician leadership: Enhancing the career development of academic physician administrators and leaders. Acad Med 2004;79:214-218.
4. Howell LP, Hogarth M, Anders TF. Creating a mission-based reporting system at an academic health center. Acad Med 2002;77:130-138.
Ms Conlon is director of the Department of Obstetrics and Gynaecology at the University of British Columbia, on site at BC Women’s Hospital and Health Centre in Vancouver. Mr Tharani was a senior business analyst in the Information Management/Information Technology Department of the Provincial Health Services Authority during the development of PhAIS and now works as a private consultant.