Diagnosis and treatment of dyslipidemia in patients with diabetes mellitus
Issue: BCMJ,
vol. 44 , No. 4 , May 2002 ,
Pages 196-202 Clinical Articles
Increased levels of serum triglycerides and decreased HDL-cholesterol are characteristic lipid abnormalities not only in patients with type II diabetes but also in people with impaired glucose tolerance. In an analysis of risk factors for coronary artery disease in non-insulin dependent diabetes mellitus (the UK Prospective Diabetes Study) the lipid abnormalities were most predictive of future coronary events. Both lifestyle and drug treatment of these abnormalities has been proven effective in reducing morbidity and mortality in well-designed clinical trials. Lifestyle changes and drug treatment (metformin, possibly statins) may prevent the onset of diabetes in patients at high risk. As visceral obesity has been associated with numerous factors believed to cause diabetes, prevention and treatment of excessive abdominal fat accumulation is a public health priority.
By diagnosing and treating lipid abnormalities in patients with diabetes, we can significantly improve their health and increase their lifespan.
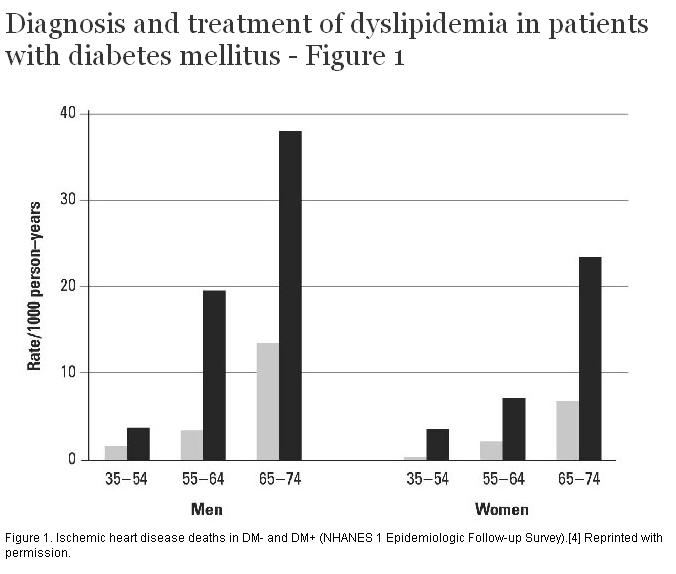
It has been predicted that up to 100 million people will be newly diagnosed with diabetes over the next year.[1] The sedentary lifestyle of wealthy populations appears to play a major role in the development of a cluster of risk factors including abdominal obesity, insulin resistance, dyslipidemia, and hypertension (metabolic syndrome X). These factors are associated with accelerated atherosclerosis seen particularly in patients with diabetes.[2,3] Approximately 80% of patients with adult onset diabetes die from consequences of atherosclerosis, namely coronary heart disease (CHD) and stroke. Figure 1 shows the data from the National Health and Nutrition Survey (NHANES) that compared CHD death rates in both men and women with and without diabetes.[4] At all ages the CHD rate in patients with diabetes was greater than in individuals without diabetes. Approximately 50% of patients with newly diagnosed diabetes already have coronary artery disease. Furthermore, a recent study by Haffner and colleagues showed that having adult onset diabetes carries the same cardiovascular risk as having had a previous coronary event.[5]
Interestingly, diabetic women have 2.5 times greater risk of CHD death compared to diabetic men.[6] Nevertheless, the absolute levels of CHD mortality remain higher in men (see ). Disturbances in triglyceride metabolism (see “Lipid abnormalities associated with insulin resistance in type II diabetes,” below) or possibly the changes in response to endothelium-dependent vasodilation due to diabetes in women and men[7] may explain the higher risk seen in women.
Not only are patients with diabetes more likely to develop CHD, but they also have higher mortality (1.5-fold) and morbidity following acute events and a high incidence of congestive heart failure. Approximately 44% of men and 37% of women with diabetes die within a year of their first MI.[8]
Subclinical disease, demonstrated by increased intima media thickness of common carotid artery, appears early in patients with diabetes[9] and it is the major determinant of subsequent clinical events.[10] Therefore, due to the long-lasting presence of metabolic syndrome in most patients with type II diabetes, it is not surprising that half of them already have CHD at the time of diagnosis of diabetes.
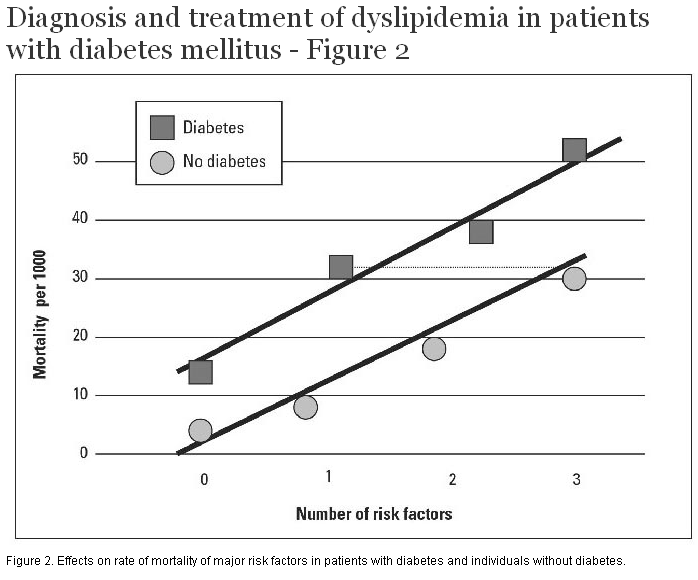
Factors predisposing to macrovascular disease in patients with diabetes
Patients with diabetes are at higher risk for macrovascular disease at all levels of risk factors (Figure 2). Of the major causal risk factors (age, smoking, hypertension, diabetes, and dyslipidemia), the last will be the major focus of this brief review.
Lipid abnormalities associated with insulin resistance in type II diabetes
Three major studies, San Antonio,[11] United Kingdom Prospective Diabetes Study (UKPDS), [12] and the Cardiovascular Health Study[8,13] showed that the major lipoprotein abnormalities in type II diabetics are an increase in serum triglycerides and decrease in HDL-cholesterol. Furthermore, serum triglycerides and HDL-cholesterol abnormalities are present not only in patients with type II diabetes but also in people with impaired glucose tolerance. In a study of aboriginal Americans,[14] the Strong Heart Study, serum HDL-cholesterol and apolipoprotein AI were decreased in those with diabetes. In this study the LDL-cholesterol levels were lower but the low- density lipoprotein particles were smaller and denser, and serum apolipoprotein B levels higher, particularly in diabetic women. We have made similar observations in a study of 250 patients with type II diabetes, that apo B levels were high in one-third of them, in fact as high as those seen in patients with heterozygous familial hypercholesterolemia.[15]
The hierarchy of risk factors for vascular disease in patients with diabetes
In an analysis of risk factors by Turner and colleagues,[16] the order of importance for prediction of future coronary events in a baseline assessment was:
1. Serum LDL-cholesterol levels
2. Serum HDL-cholesterol levels
3. Hemoglobin A1C
4. Systolic blood pressure
5. Smoking
Coagulation abnormalities associated with insulin resistance. Numerous abnormalities of coagulation, fibrinolysis, and platelet function have been described in patients with diabetes (Table). These and other risk factors likely interact in a synergistic fashion. Moss and colleagues demonstrated that coagulation and lipid abnormalities contribute together to recurrent coronary events.[17] Increased levels of D-dimer, if present, together with high serum apo B and low apo AI levels, increased the hazard ratio to 8.4 compared to hazard ratios for the individual risk factors (i.e., high D-dimer, high apo B, or low apo AI) that ranged between 1.5 and 2.5. Similar findings were reported in a study of Factor V Leiden and prothrombin 20210A in combination with other risk factors.[18]
Increased serum concentration of vascular cell adhesion molecule 1 was also associated with CHD mortality.[19] Furthermore, C-reactive protein (CRP) is also increased in patients with diabetes (see below “Statins and the development of diabetes,”). Finally, high levels of homocysteine were associated with mortality in patients with diabetes.[20]
Effect of lipid-lowering treatment on vascular events in patients with diabetes
A number of large studies that used fibrates or statins also included patients with diabetes. However, the only trial specifically aimed at men and women with type II diabetes has been the Diabetes Atherosclerosis Intervention Study (DAIS), an angiography-reangiography study with 418 men and women randomized to either fenofibrate micronized 200 mg per day or placebo.[21] DAIS was an international project with centres in Canada (including Vancouver), Scandinavia, and France. On average the participants were followed for 3 years. As expected, all of them had at least one visible lesion on coronary angiography at the baseline and one-half of them were previously diagnosed with clinical coronary heart disease. The endpoints were changes in minimum lumen diameter, mean segment diameter, and mean percent stenosis.
Fenofibrate decreased plasma triglycerides (-29%), increased HDL-cholesterol (+7%), and decreased LDL-cholesterol (-6%). All these changes were statistically significant. While there was no significant change in mean segment diameter that indicates diffused disease progression, the treatment group had a statistically significant 40% reduction in the disease progression assessed by minimum lumen diameter and 42% decrease by percentage of change in mean stenosis (p = 0.029 and 0.02, respectively). In regard to the composite clinical endpoints, there were 38 events in the treated and 50 in the placebo group. Albeit not statistically significant, the reduction in events was similar to that seen in patients with diabetes in other trials (DAIS = 23%, VA-HIT = 24%, LIPID = 19%, CARE = 25%, 4S = 55%). It is also noteworthy that the changes in the above angiographic parameters were similar to those observed in patients without diabetes in other trials.[22]
Outcome studies with subgroups of patients with diabetes
In the Helsinki Heart Study[23] a subgroup of gemfibrozil treated patients with type II diabetes showed a non-significant reduction in CHD compared with the placebo group. In another trial that used gemfibrozil, namely the VA-HIT Study,[24] there was a similar reduction in cardiovascular events in patients with and without diabetes. However, in the group of patients with diabetes the difference was statistically borderline at p = 0.052 (compared to the overall relative risk reduction significance at p<0.001). Of interest is the fact that in this study there was no change in the mean values for LDL-cholesterol, a 6% increase in HDL-cholesterol, and 31% decrease in serum triglyceride concentration.
Of the studies that used statins, the subgroup analysis of the 5% of patients in the Scandinavian Simvastatin Survival Study (4S) who had diabetes showed a marked reduction in LDL-cholesterol and an increase in HDL-cholesterol resulted in a significant reduction of risk for coronary events, all vascular events, and mortality in these patients.[25] In addition, those with impaired fasting glucose also benefited from the treatment. Altogether, there was an impressive 55% reduction in coronary events (p = 0.002) in this subgroup. It is important to remember, however, that these patients were selected based on very high LDL levels and had relatively low triglyceride levels (<2.5 mmol/L).
In the Intervention with Pravastatin in Ischaemic Disease (LIPID) study there was a mean risk reduction in the subgroup with diabetes in the active treatment group, but the findings were not statistically significant.[26] Another pravastatin study, Cholesterol and Recurrent Events (CARE), showed similar trends toward risk reduction in a subgroup of patients with fasting glucose both less than and greater than 6 mmol/L. Here the findings were only significant when all the endpoints were combined into expanded endpoints.[27] In the Post Coronary Artery Bypass Graft Study[28]—which examined aggressive versus moderate reduction of LDL-cholesterol (targets 3.4 mmol/L to 3.6 mmol/L versus 1.5 mmol/L to 2.2 mmol/L)—there was also a trend toward less progression of the lesion in coronary artery bypass grafts and less occlusion in the subgroup of patients with diabetes who were treated aggressively. However, the results once again did not reach statistical significance. Finally, in the recently presented UK Heart Protection Study,[29] patients with diabetes both with and without coronary artery disease benefited significantly from treatment with 40 mg of simvastatin. Importantly, even individuals with initial levels of LDL-cholesterol below 2.6 mmol/L had significantly lower morbidity and mortality with the statin treatment, which caused, on average, 1 mmol/L decrease in LDL-cholesterol. This finding will likely change our treatment targets for the very high-risk groups, which includes patients with diabetes and those with established coronary artery disease.
Statins and the development of diabetes
Recent reports suggest that statins may delay or prevent the development of diabetes.[30,31] A 30% decrease in the likelihood of developing diabetes was observed with pravastatin (WOSCOP) and lovastatin (AFCAPS/TEXCAPS) treatment. Possible explanations of these effects include the triglyceride and anti-inflammatory lowering effect of statins (decreases in CRP, interleukin 6, and P-selectin) and the direct effects of statins on endothelial function. The prevention of the onset of diabetes by statins may be independent of their lipid-lowering effects.
Prevention of type II diabetes by changes in lifestyle
Lifestyle intervention (diet and exercise) in a group of 522 men and women with impaired glucose tolerance was shown to generate an impressive 58% reduction of risk in diabetes.[32] The decrease in the incidence of diabetes was directly related to decreases in weight, waist circumference, blood pressure, serum lipids, and serum glucose. These results have been confirmed in a larger study by the Diabetes Prevention Program Research Group.[33] This study also showed that metformin reduced the incidence of diabetes, and that lifestyle was more effective than metformin.
Lipid management in patients with metabolic syndrome and/or type II diabetes
Measurement of serum fasting lipids (total cholesterol, triglycerides, HDL, and calculated LDL-cholesterol) is essential for diagnosing a lipid abnormality. However, adding a apolipoprotein B measurement is important as our recent finding demonstrated (see “Lipid abnormalities associated with insulin resistance in type II diabetes,” above). The targets for patients with diabetes are LDL-cholesterol below 2.5 mmol/L, ratio of total to HDL-cholesterol below 4 and triglyceride level below 2 mmol/L (some studies suggest that triglyceride below 1.5 mmol/L is an ideal level at which the likelihood of small, dense LDL particles to predominate is very low). The target level for apo B based on the above is ≤0.9 g/L. Apo B indicates the particle number, and at the concentrations below 0.9 g/L the particle number of LDL is relatively low. Patients with diabetes may have a “normal” level of LDL-cholesterol, but because of a predominance of a larger number of atherogenic small, dense LDL particles, they are still at high risk.
Based on recent reports, measurement of C-reactive protein may also be of value in patients with normal lipid levels.[34] Thus, in very high-risk patients who have normal lipid profiles, statin treatment may still be indicated if serum C-reactive protein is over 3 mg/L.
The benefit of improved glycemic control for reducing cardiovascular events is controversial. The UKPDS study[12] showed a 16% decrease in cardiovascular risk for every 0.9% reduction in hemogblobin A1C. This same study, however, failed to show a reduction in cardiovascular events with improved glycemic control. This has led to the notion that other factors, such as blood pressure and lipids, play a greater role in the pathogenesis of atherosclerosis in diabetics. Metformin, even at low doses (i.e., 500 mg bid) will reduce triglycerides.[35] The newest class of insulin sensitizers, the thiazinediones, have a number of effects on lipids, including a decrease in triglycerides, increase in HDL-C, and at least initially, an increase in LDL-cholesterol.[36-38] The effect of thiazinediones on lipids depends on a number of factors, including the degree of dysglycemia and the severity of the dyslipidemia. Surrogate markers of increased risk for atherosclerosis such as carotid artery intimal media thickness[39] and PAI-I[40] are decreased with thiazinedione therapy. Ultimately, the utility of insulin sensitizers in the treatment of diabetic-associated atherosclerosis will require clinical outcome trials.
There is little doubt that modifications in exercise and diet should be the primary tools in the management of the metabolic syndrome and diabetes. Concentrating on a reduction in abdominal obesity—which is related to higher CRP values and early increases in intima media thickness of carotids—will improve the management of these individuals.[41] After instructions for waist circumference measurements are given, patients should be told to concentrate on their waist measurement rather than their weight. Among many beneficial effects of exercise are a decrease in blood pressure, improved lipid profile, and improved mood and general well-being. All this should be emphasized to patients when suggesting the most practical routine, namely a daily 30-minute walk at a brisk pace (1.5 kilometres in 15 minutes).
In patients with diabetes, either fibrates or statins can be used to achieve the lipid targets depending on the primary lipid abnormality (i.e., LDL-C <2.5, TG <2.0 mmol/L ad TC/HDL-C ratio <4 mmol/L). Based on the UK Heart Protection Study, our lipid targets will likely be lowered (by another 1.0 mmol of LDL-cholesterol, that is, to levels closer to 1.5 mmol/L for LDL-cholesterol). Combinations of statins and fibrates may be necessary in some of these patients. With the exception of the cerivastatin-gemfibrozil combination, the statin fibrate and statin niacin combinations are relatively safe. The best precaution is to tell patients to quit the medications (there is no penalty in quitting abruptly) if any untoward symptoms appear, monitoring AST and CK initially at 6 weeks and afterward at 6-month intervals, and perhaps (anecdotally proven) use of coenzyme Q10 (30 mg to 60 mg a day) for minor muscle aches. In symptomatic patients, lipid-lowering medications should be discontinued or adjusted if the CK or the AST exceed three times the upper limit of the reference-range value.
In the recent HATS Study,[42] the combination of simvastatin and niacin was fairly well-tolerated by patients with diabetes. While niacin can be used in these patients, a significant percentage will need adjustment of their glucose-lowering regimen. Newer formulations of niacin such as Niaspan may be more useful in patients with diabetes.
The diagnosis and treatment of lipid abnormalities in patients with diabetes will significantly decrease their morbidity and mortality. Lifestyle changes and treatment with statins may prevent the onset of diabetes in patients at high risk. As obesity has been associated with numerous factors believed to cause diabetes, prevention and treatment of excessive accumulation of abdominal fat is a public health priority.
None declared.
Table. Platelet and coagulation/fibrinolytic abnormalities in patients with diabetes.
|
Alterations of platelets Abnormalities of platelet function Abnormalities of coagulation |
References
1. Zimmet P. Diabetes epidiology as a tool to trigger diabetes research and care. Diabetologia 1999;42:499-518.PubMed Citation
2. Lehto S, Ronnemaa T, Pyorala K, et al. Cardiovascular risk factors clustering with endogenous hyperinsulinaemia predict death from coronary heart disease in patients with Type II diabetes. Dioabetologia 2000;43:148-155.PubMed Abstract
3. Pyorala M, Miettinen H, Halonen P, et al. Insulin resistance syndrome predicts the risk of coronary heart disease and stroke in healthy middle-aged men: The 22-year follow up results of the Helsinki Policemen Study. Arterioscler Thromb Vasc Biol 2000;20:538-544.PubMed Abstract Full Text
4. Gu K, Cowie CC, Harris MI. Diabetes and decline in heart disease mortality in US adults. JAMA 1999;281:1291-1297.PubMed Abstract
5. Haffner SM, Lehto S, Ronnemaa T, et al. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339:229-234.PubMed Abstract Full Text
6. Lee WL, Cheung AM, Cape D, et al. Impact of diabetes on coronary artery disease in women and men: A meta-analysis of prospective studies. Diabetes Care 2000;23:962-968.PubMed Abstract Full Text
7. Steinberg HO, Paradisi G, Cronin J, et al. Type II diabetes abrogates sex differences in endothelial function in premenopausal women. Circulation 2000;101:2040-2046.PubMed Abstract Full Text
8. Psaty BM, Furbert CD, Kuller LH, et al. Traditional risk factors and subclinical disease measures as predictors of first myocardial infarction in older adults: The Cardiovascular Health Study. Arch Intern Med 1999;159:1339-1347.PubMed Abstract
9. Haffner SM Agnostino RD, Saad MF, et al. Carotid artery atherosclerosis in type-2 diabetic and nondiabetic subjects with and without symptomatic coronary artery disease (The Insulin Resistance Atherosclerosis Study). Am J Cardiol 2000;85:1395-1400.PubMed Abstract
10. Kuller LH, Velentgas P, Barzilay J, et al. Diabetes mellitus: Subclinical cardiovascular disease and risk of incident cardiovascular disease and all-cause mortality. Arterioscler Thromb Vasc Biol 2000;20:823-829.PubMed Abstract Full Text
11. Mahaney MC, Blangero J, Comuzzie AG, et al. Plasma HDL cholesterol, triglycerides and adiposity. A quantitative genetic test of the conjoint trait hypothesis in the San Antonio Family Heart Study. Circulation 1995;92:3240-3248.PubMed Abstract Full Text
12. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK prospective Diabetes Study (UKPDS) Group [published erratum appears in Lancet 1999;354:602]. Lancet 1998;352:837-853.PubMed Abstract
13. Kuller L, Borhani N, Furbert C, et al. Prevalence of subclinical atherosclerosis and cardiovascular disease and association with risk factors in the Cardiovascular Health Study. Am J Epidemiol 1994;139:1164-1179.PubMed Abstract
14. Howard BV, Robbins DC, Sievers ML, et al. LDL cholesterol as a strong predictor of coronary heart disease in diabetic individuals with insulin resistance and low LDL: The Strong Heart Study. Arterioscler Thromb Vasc Biol 2000;20:830-835.PubMed Abstract Full Text
15. Sniderman A, Lamarche B, Seccombe D, et al. Hypertriglyceridemic HyperapoB in type II diabetes. Diabetes Care. 2002;25:579-582.PubMed Abstract
16. Turner RC, Millns H, Neil HA, et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS:23). BMJ 1998;316:823-828.PubMed Abstract Full Text
17. Moss AJ, Goldstein RE, Marder VJ, et al. Thrombogenic factors and recurrent coronary events. Circulation 1999;99:2517-2522.PubMed Abstract Full Text
18. Doggen CJM, Cats VN, Bertina RM, et al. Interaction of coagulation defects in cardiovascular risk factors. Circulation 1998;97:1037-1041.PubMed Abstract Full Text
19. Jager A, van Hinsbergh VW, Kostense PJ, et al. Increased levels of soluble vascular cell adhesion molecule 1 are associated with risk of cardiovascular mortality in type 2 diabetes: The Hoorn study. Diabetes 2000;49:485-491.PubMed Abstract Full Text
20. Hoogeveen EK, Kosense PJ, Jakobs C, et al. Hyperhomocysteinemia increases risk of death, especially in type 2 diabetes: 5-year follow up of the Hoorn study. Circulation 2000;101:1506-1511.PubMed Abstract Full Text
21. Diabetes Atherosclerosis Intervention Study Investigators. Effect of fenofibrate on progression of coronary artery disease in type 2 diabetes: The Diabetes Atherosclerosis Intervention Study, a randomised study. Lancet 2001;357:905-910.PubMed Abstract
22. Waters D. Lessons from coronary atherosclerosis “regression” trials. Clin Cardiol 1996;14:31-50.PubMed Abstract
23. Frick MH, Haapa K, Heinonen OP et al. Helsinki Heart Study: Primary prevention trial with gemfibrozil in middle-aged men with dyslipidemia: Safety and treatment, changes in risk factors and incidence of coronary heart disease. N Engl J Med 1987;317:1237-1245.PubMed Abstract
24. Rubins HB, Robins SJ, Collins D et al. Gemfibrozil for the secondary prevention of coronary artery disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med 1999;341:410-418.PubMed Abstract Full Text
25. Haffner SM, Alexander CM, Cook TJ et al. Reduced coronary events in simvastatin-treated patients with coronary heart disease and diabetes or impaired fasting glucose levels: Subgroup analyses of the Scandinavian Simvastatin Survival Study. Arch Int Med 1999;159:2661-2667. PubMed Abstract
26. The Long Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med 1998;339:1349-1357.PubMed Abstract Full Text
27. Sacks FM, Moye LA, Davis BR, et al. Relationship between plasma LDL concentrations during treatment with pravastatin and recurrent coronary events in the Cholesterol and Recurrent Events trial. Circulation 1998;97:1446-1452.PubMed Abstract Full Text
28. Hoogwerf BJ, Waness A, Cressman M, et al. Effects of aggressive cholesterol lowering and low-dose anticoagulation on clinical and angiographic outcomes in patients with diabetes: The Post Coronary Artery Bypass Graft Trial. Diabetes 1999;48:1289-1294.PubMed Abstract Full Text
29. Collins R, Baigent C, Peto R, et al. Presented at the American Heart Association meeting, Anaheim, CA, November 2001.
30. Freeman DJ, Norrie J, Sattar N, et al. Pravastatin and the development of diabetes mellitus. Evidence for a protective treatment effect in the West of Scotland Coronary Prevention Study. Circulation 2001;103:357-362.PubMed Abstract
31. Gotto AM Jr. Lipid management in patients at moderate risk for coronary heart disease: Insights from the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS). Am J Med 1999;107(2A):36S-39S.PubMed Abstract
32. Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001;344:1343-1350.PubMed Abstract Full Text
33. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346:393-403.PubMed Abstract
34. Ridker PM, Rifai N, Clearfield M, et al. Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events. N Engl J Med 2001;344:1959-1965.PubMed Abstract Full Text
35. Executive summary of the Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-2497.PubMed Citation
36. Ghazzi MN, Perez JE, Antonucci TK et al. Cardiac and glycemic benefits of troglitazone treatment in NIDDM. The Troglitazone Study Group. Diabetes 1997;46:433-439.PubMed Abstract
37. Lebovitz HE, Dole JF, Patwardhan R et al. Rosiglitazone monotherapy is effective in patients with type 2 diabetes. Clin Endocrinol Metabol 2001;86:280-288.PubMed Abstract
38. Aronoff S, Rosenblatt S, Braithwaite S, et al. Pioglitazone hydrochloride monotherapy improves glycemic control in the treatment of patients with type 2 diabetes: a 6-month randomized placebo-controlled dose-response study. The Pioglitazone 001 Study Group. Diabetes Care 2000;23:1605-1611.PubMed Abstract Full Text
39. Minamikawa J, Tanaka S, Yamauchi M, et al. Potent inhibitory effect of troglitazone on carotid arterial wall thickness in type 2 diabetes. J Clin Endocrinol Metabol 1998;83:1818-1820.PubMed Abstract] Full Text
40. Kruszynska YT, Yu JG, Olefsky JM, et al. Effects of troglitazone on blood concentrations of plasminogen activator inhibitor 1 in patients with type 2 diabetes and in lean and obese normal subjects. Diabetes 2000;49:633-639.PubMed Abstract Full Text
41. Despres JP, Lemieux I, Prud’homme D. Treatment of obesity: Need to focus on high risk abdominally obese patients. BMJ 2001;322:716-720.PubMed Citation Full Text
42. Brown BG, Zhao X, Chait A, et al. Niacin plus simvastatin but not antioxidant vitamins, protect against atherosclerosis and clinical events in CAD patients with low HDL-C. Scientific Sessions Abstract #2461, Circulation 2000;102,II-1-II-1045.
Jiri Frohlich MD, FRCPC and Greg Bondy MD, FRCPC
Dr Frohlich is academic director of St. Paul’s Hospital Healthy Heart Program/Lipid Clinic and professor of pathology and laboratory medicine at the University of British Columbia. Dr Bondy is associate director of St. Paul’s Hospital Healthy Heart Program/Lipid Clinic and an associate clinical professor in the Department of Pathology and Laboratory Medicine, University of British Columbia.

{kind=link}
{kind=link}