Carotid artery stenting by a cardiovascular services department in Canada
Issue: BCMJ,
vol. 51 , No. 4 , January February 2009 ,
Pages 14-19 Clinical Articles
Background: Patients with ischemic heart disease often have concomitant carotid artery disease. In appropriately selected patients, carotid artery stenting has been considered as an alternative to carotid endarterectomy. In the US and Europe, cardiologists are the dominant workforce to perform carotid artery stenting. The objective of this study was to assess the feasibility and safety of carotid artery stenting performed at a tertiary cardiovascular centre in Canada.
Methods: 50% stenosis, or asymptomatic >80% stenosis in the carotid artery.
Results: Between July 2005 and January 2008, 100 patients underwent carotid artery stenting. The study population included a broad spectrum of symptomatic and asymptomatic patients, high- or average-risk for surgical endarterectomy, and those who were waiting for open-heart surgery. All but 1 patient had procedural success. There was 1 periprocedural stroke and 1 myocardial infarction 3 days after the procedure. No patient died within 30 days. All patients completed 6-month follow-up; 98% completed 1-year follow-up. Between 1 month and 1 year after the procedure, 1 patient had target lesion revascularization, and there were 5 deaths, including 4 cardiac deaths and 1 sudden death, which was presumed cardiac related.
Conclusions: A carotid artery stenting program established by a tertiary care cardiovascular department in Canada is feasible. It provides clinical outcomes that meet the benchmark established by the current practice guidelines.
The experience of the cardiovascular services department at Royal Columbian Hospital confirms the safety and effectiveness of carotid artery stenting—a less invasive alternative to carotid endarterectomy for carotid revascularization.
Background
Interventional cardiologists possess many of the required skills for managing the concomitant carotid and coronary atherosclerotic disease common in cardiology practice.[1,2] For the past 3 decades, carotid endarterectomy (CEA) has been the standard intervention for patients with symptomatic disease and more than 50% stenosis, and for patients with asymptomatic disease and more than 80% stenosis, provided the perioperative risk has satisfied the benchmark established by the guidelines.[3] Carotid artery stenting (CAS) has been accepted as an alternative to CEA in the treatment of patients with symptomatic, and in some cases asymptomatic, obstructive extracranial carotid artery disease.[4-7] While neuroradiologists have traditionally been responsible for invasive cerebrovascular imaging and interventional therapy in Canada, other countries have relied upon cardiologists to provide CAS, as demonstrated in the most recent CAPTURE study,8 which found that 55% of CAS procedures were done by cardiologists and 22% by vascular surgeons at major US and European centres.[8,9] Furthermore, patients with complex disease often benefit from treatment by specialists who have expertise in both cerebral and cardiovascular disease management. With these potential advantages in mind, we undertook a study to consider the feasibility and safety of providing CAS at a tertiary care cardiovascular department.
Methods
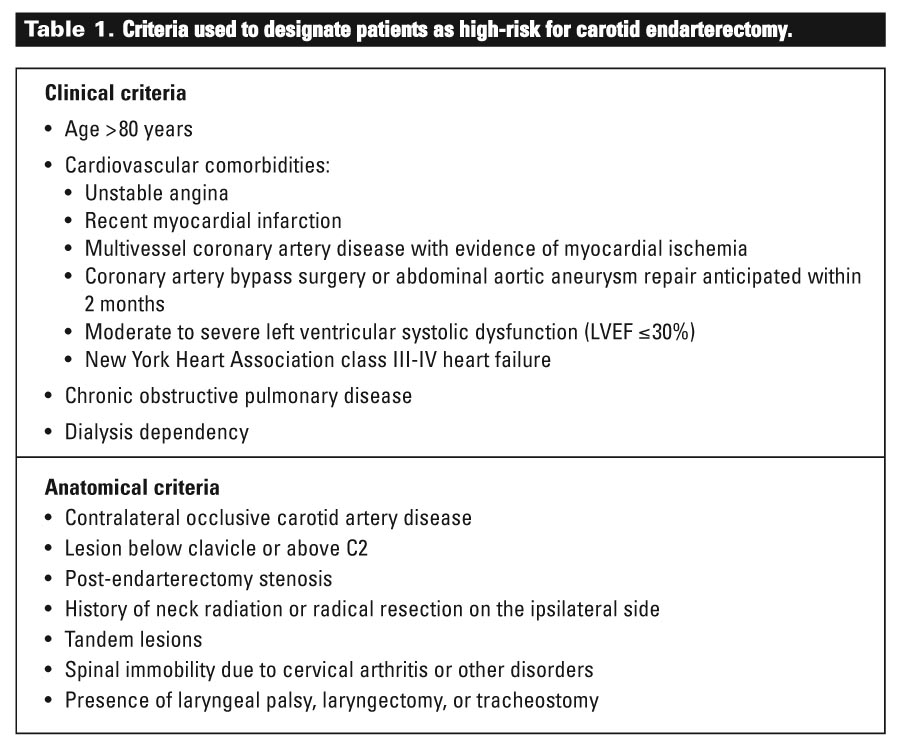
Baseline characteristics, procedural data, and postprocedural follow-up data were collected prospectively for the patients undergoing CAS in the cardiac catheterization laboratory at Royal Columbian Hospital starting in July 2005. Patients who had symptomatic or asymptomatic severe obstructive extracranial carotid artery disease and were designated high-risk for CEA were considered suitable for CAS [Table 1]. Patients who were at average risk but preferred the less invasive procedure were also considered suitable for CAS. All patients who had a recent transient ischemic attack or stroke were seen and examined by a neurologist to document preprocedural neurological findings and to assess neurological reserve before proceeding to CAS. Noninvasive imaging modalities, including carotid duplex ultrasonography, magnetic resonance angiography, and computed tomography of the brain, were used prior to CAS.
{kind=link}
The procedural technique of CAS has been described previously.[1] CAS was considered for symptomatic patients who were confirmed on invasive angiography to have more than 50% stenosis, and for asymptomatic patients confirmed to have more than 80% stenosis, according to the criteria established in the North American Symptomatic Carotid Endarterectomy Trial.[10] Procedural success was defined by stent implantation resulting in less than 30% residual luminal narrowing. Following the procedure, patients were observed overnight on the cardiology ward before discharge. Aspirin was prescribed for life and clopidogrel was prescribed for 1 month. Patients who required urgent cardiac surgery were kept in the hospital until surgery and clopidogrel was withheld from these patients for 5 days before surgery. Blood pressures were controlled meticulously under a strict protocol. Systolic blood pressures were controlled within the range of 90 to 120 mmHg after bilateral CAS or unilateral CAS with contralateral occlusion, or within 90 to 140 mmHg after unilateral CAS with patent contralateral carotid artery. Along with postprocedural intravenous fluid infusion, adjunctive intravenous nitroglycerin, low-dose dopamine, or oral pseudoephedrine were administered as needed. Oral antihypertensive medications were adjusted by the cardiologist prior to discharge. After discharge, patients were instructed to monitor themselves and report any hypertension to the operating physician within the first week. They were also asked to report any headache or neurological symptoms.
Clinical follow-up was performed within the first month of the procedure and surveillance ultrasound appointments were scheduled at 6 months, at 1 year, and on a yearly basis after the index procedure.
Results
From 28 July 2005 to 31 January 2008, a total of 100 patients underwent CAS in the catheterization laboratory to treat 110 carotid lesions, including 10 patients who underwent bilateral CAS. Of these patients, 55 were male and 45 were female, with a mean age of 72.0 (SD 8.6) years.
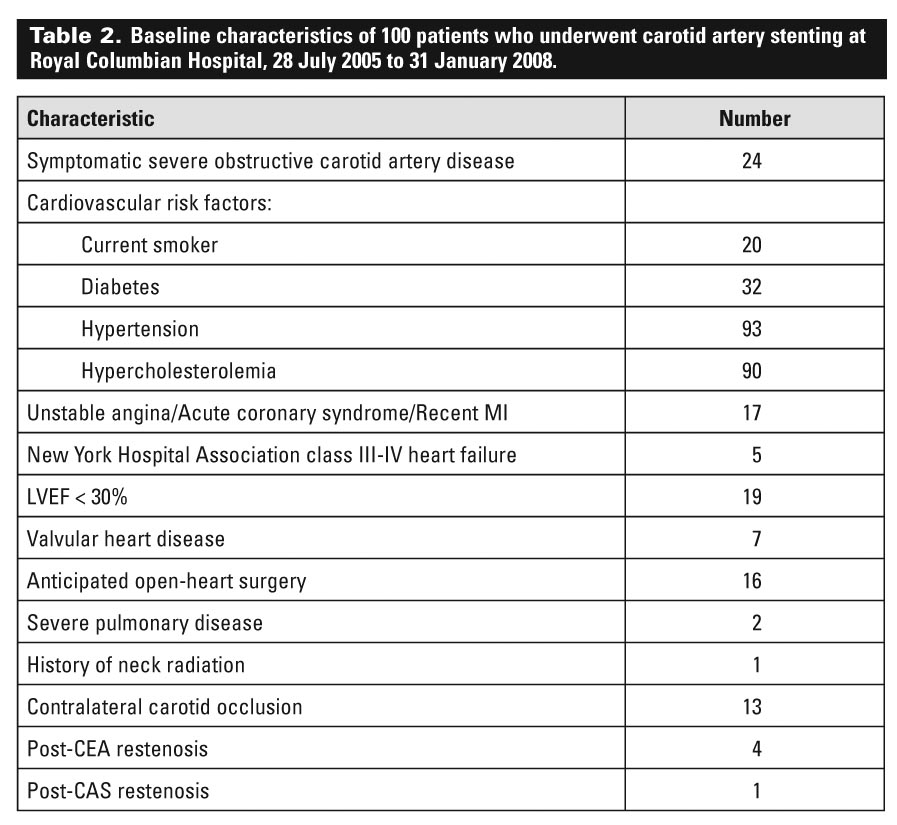
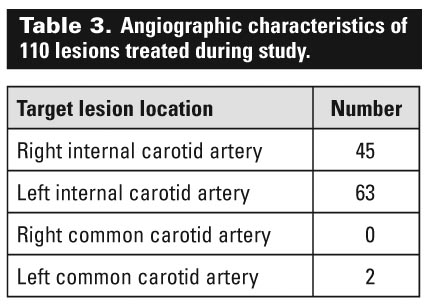
The baseline clinical and angiographic characteristics of the patients are shown in [Table 2] and [Table 3]. The comorbidities were typical for patients in a cardiovascular practice. Of note, 24 of the 100 patients were symptomatic (that is, they had experienced recurrent transient ischemic attack or ipsilateral stroke within 6 months of the procedure), similar to the populations enrolled in most CAS preapproval trials and registries. In addition, 63 of the patients met at least one of the high-risk criteria for carotid endarterectomy, including 17 patients who had experienced a recent acute coronary syndrome or myocardial event, 16 who were waiting for open-heart surgery, and 19 who had a left ventricular ejection fraction of less than 30%.
{kind=link}
{kind=link}
The mean preprocedural stenosis of the target lesion was 83.0% (SD 8.1%), and the mean stenosis after CAS was 4.1% (SD 10.7%). While undergoing CAS, some patients also underwent diagnostic coronary angiography (22 patients), coronary angioplasty (4), renal angioplasty (4), and subclavian angioplasty (2).
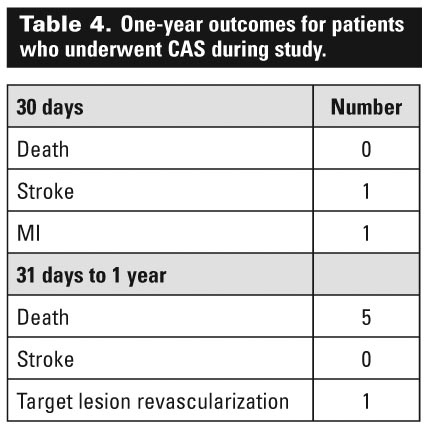
The 30-day and 1-year outcomes are shown in [Table 4] . All procedures except one were successful. The unsuccessful procedure was related to a heavily calcified obstructive internal carotid artery (ICA) lesion that could not be crossed, even with a 0.014-inch hydrophilic coronary guidewire. The patient had contralateral ICA occlusion. She later underwent uneventful elective carotid endarterectomy.
{kind=link}
The single case associated with periprocedural stroke involved an 81-year-old woman who had a history of multiple strokes and developed slow-flow state immediately after dilation of the stent. Following one pass of the thrombo-aspiration catheter and the retrieval of the filter emboli-protection device, normal flow was achieved within the extracranial and intracranial cerebral arteries without evidence of embolization on the angiogram. Although the patient remained dysphasic and hemiplegic for several days, she gradually recovered and had no residual neurological deficit at 5-month follow-up.
Hyperperfusion syndrome occurred in one case after an apparently successful CAS for unilateral carotid stenosis. The symptom resolved with intravenous mannitol and the patient was discharged 48 hours after the procedure.
The outcomes were consistent with the benchmark of carotid revascularization established by the American College of Cardiology and the American Heart Association, and in clinical trials [Figure].[3,4] All patients completed 6-month follow-up; 98% completed 1-year follow-up. Five deaths occurred between 1 month and 1 year. These included 4 cardiac deaths and 1 sudden death; all patients who died had a history of coronary artery disease.
Discussion
Our prospective registry demonstrates the feasibility and safety of adopting cerebral angiography and carotid stenting as a standard procedure in the cardiac catheterization laboratory in this country.
The only periprocedural stroke in this study cohort took place in an octogenarian with symptomatic ICA disease. Indeed, age beyond 80 years and the presence of a symptomatic carotid lesion are two traditional risk factors associated with increased risk of periprocedural stroke with CAS. This may be because octogenarians have a low cerebrovascular reserve and cannot tolerate even a small insult with microemboli to the brain. Another possible reason for the increased risk may be the soft and inflamed plaque characteristic of symptomatic carotid artery lesions. This plaque tends to be thrombogenic and may be associated with slow flow after stent deployment, as suggested by one large prospective registry study.[11]
Dilation of a stent to achieve minimal residual luminal narrowing is crucial for reducing restenosis risk, but it is also the step where slow flow and periprocedural stroke can take place during CAS. Perhaps a more conservative balloon sizing for stent dilation should be adopted in octogenarians and for symptomatic carotid artery stenosis to minimize the risk of periprocedural stroke.
Several subgroups in our patient population merit further consideration. The first group includes those patients who require carotid revascularization prior to cardiac surgery. While the appropriate management strategy for these patients has not been defined, the risk of stroke during cardiac surgery is significantly elevated among patients with severe internal carotid artery disease without adequate intracranial collateralization through the Circle of Willis. CEA prior to, or combined with, coronary bypass surgery is associated with an unacceptably high risk of stroke and cardiovascular morbidity.[12-14] Consistent with recently reported results,[15,16] our experience suggests that CAS prior to open-heart surgery is safe and effective for patients, including those with symptomatic left main coronary disease, critical aortic stenosis, and poor ventricular function, provided that the physician is familiar with the hemodynamic management of these patients.
While all our patients received clopidogrel prior to CAS, we withheld clopidogrel after CAS if urgent cardiac surgery was planned during the same admission. Although clopidogrel use is part of routine CAS practice at Royal Columbian based on our experience in percutaneous coronary interventions, the efficacy of this medication after CAS has not been shown in clinical trials. Theoretically, stent thrombosis is less likely to take place after CAS than after coronary stenting because of the high-flow state and large lumen diameter of the carotid artery.
Another subgroup in our study worth considering includes those patients who underwent bilateral CAS. Unlike CEA, bilateral carotid revascularization is feasible using stents. The obvious advantage of bilateral CAS lies in avoiding an additional invasive procedure. However, bilateral CAS may result in an increased risk of hyperperfusion syndrome, which is associated with significant risks of morbidity and mortality.[17-19] Through a strict blood pressure control protocol, bilateral CAS has been safely performed without increased incidence of hyperperfusion syndrome.[20] In our practice, we consider bilateral CAS in the same setting if the patient has normal renal function and does not have risk factors for hyperperfusion syndrome (that is, bilateral stenosis >90% or systolic blood pressure >180 mmHg).[19]
While cardiologists are the specialists performing CAS most commonly in the US and Europe,8 the creation of a new specialty of endovascular intervention over the past 10 to 15 years has had a significant impact on the training and practice of vascular surgery and cardiology in many centres.[21] The extraordinarily poor CAS outcomes demonstrated in the Endarterectomy Versus Stenting in Patients with Symptomatic Severe Carotid Stenosis study highlight the importance of adequate training.[22] As is the case with CEA,3 CAS should only be performed by interventionalists who can maintain the periprocedural risk of stroke at less than 6% for symptomatic patients and less than 3% for asymptomatic patients. By meeting this standard when performing CAS in cardiac catheterization laboratories, cardiovascular specialists can offer patients a viable alternative to carotid endarterectomy.
Acknowledgments
I appreciate the assistance of my colleagues Dr Kennely Ho (Department of Neuroscience, Royal Columbian Hospital) and Dr Mark Henderson (who was in the Cardiovascular Services Department, Royal Columbian Hospital, at the time of writing) for reviewing this article.
Competing interests
None declared.
References
1. Chan AW. Expanding roles of the cardiovascular specialists in panvascular disease prevention and treatment. Can J Cardiol 2004;20:535-544.
2. Chan AW, Henderson MA. Immediate catheter-directed reperfusion for acute stroke occurring during diagnostic cardiac catheterization. Catheter Cardiovasc Interv 2006;67:314-318.
3. Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: A statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation 1998;97:501-509.
4. Yadav JS, Wholey MH, Kuntz RE, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med 2004;351:1493-1501.
5. Gurm HS, Yadav JS, Fayad P, et al. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med 2008;358:1572-1579.
6. Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: Co-sponsored by the Council on Cardiovascular Radiology and Intervention: The American Academy of Neurology affirms the value of this guideline. Circulation 2006;113:e409-449.
7. Bates ER, Babb JD, Casey DE, Jr., et al. ACCF/SCAI/SVMB/SIR/ASITN 2007 clinical expert consensus document on carotid stenting: A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents (ACCF/SCAI/SVMB/SIR/ASITN Clinical Expert Consensus Document Committee on Carotid Stenting). J Am Coll Cardiol 2007;49:126-170.
8. Gray WA, Yadav JS, Verta P, et al. The CAPTURE registry: Results of carotid stenting with embolic protection in the post approval setting. Catheter Cardiovasc Interv 2007;69:341-348.
9. Wholey MH, Al-Mubarek N. Updated review of the global carotid artery stent registry. Catheter Cardiovasc Interv 2003;60:259-266.
10. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 1991;325:445-453.
11. Casserly IP, Abou-Chebl A, Fathi RB, et al. Slow-flow phenomenon during carotid artery intervention with embolic protection devices: Predictors and clinical outcome. J Am Coll Cardiol 2005;46:1466-1472.
12. Cywinski JB, Koch CG, Krajewski LP, et al. Increased risk associated with combined carotid endarterectomy and coronary artery bypass graft surgery: A propensity-matched comparison with isolated coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth 2006;20:796-802.
13. Naylor R, Cuffe RL, Rothwell PM, et al. A systematic review of outcome following synchronous carotid endarterectomy and coronary artery bypass: Influence of surgical and patient variables. Eur J Vasc Endovasc Surg 2003;26:230-241.
14. Giangola G, Migaly J, Riles TS, et al. Perioperative morbidity and mortality in combined vs. staged approaches to carotid and coronary revascularization. Ann Vasc Surg 1996;10:138-142.
15. Ziada KM, Yadav JS, Mukherjee D, et al. Comparison of results of carotid stenting followed by open heart surgery versus combined carotid endarterectomy and open heart surgery (coronary bypass with or without another procedure). Am J Cardiol 2005;96:519-523.
16. Van der Heyden J, Suttorp MJ, Bal ET, et al. Staged carotid angioplasty and stenting followed by cardiac surgery in patients with severe asymptomatic carotid artery stenosis: Early and long-term results. Circulation 2007;116:2036-2042.
17. Chen MS, Bhatt DL, Mukherjee D, et al. Feasibility of simultaneous bilateral carotid artery stenting. Catheter Cardiovasc Interv 2004;61:437-442.
18. Henry M, Gopalakrishnan L, Rajagopal S, et al. Bilateral carotid angioplasty and stenting. Catheter Cardiovasc Interv 2005;64:275-282.
19. Abou-Chebl A, Yadav JS, Reginelli JP, et al. Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: Risk factors, prevention, and treatment. J Am Coll Cardiol 2004;43:1596-1601.
20. Abou-Chebl A, Reginelli J, Bajzer CT, et al. Intensive treatment of hypertension decreases the risk of hyperperfusion and intracerebral hemorrhage following carotid artery stenting. Catheter Cardiovasc Interv 2007;69:690-696.
21. Gray WA. Proceedings of the TCT: Endovascular interventional care evolves into multidisciplinary field. J Interv Cardiol 2006;19:222-225.
22. Mas JL, Chatellier G, Beyssen B, et al. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med 2006;355:1660-1671.
Dr Chan is a staff cardiologist in the Department of Cardiovascular Services at Royal Columbian Hospital, New Westminster, British Columbia.