A study of information technology use and implementation of electronic medical record systems in BC medical practices
Issue: BCMJ,
vol. 51 , No. 5 , April 2009 ,
Pages 114-121 Clinical Articles
Background: The use of information technology (IT) and electronic medical records (EMRs) in medical offices can improve health care delivery. In 2006 funding was approved to support the implementation of EMR systems in BC through the Physician Information Technology Office (PITO). In order to answer questions about current EMR use and physician readiness for adoption, a study was proposed to update the status of IT use by BC physicians and provide a detailed profile of early adopter EMR users.
Methods: Eligible BC physicians were contacted in late 2007 and asked to participate in a survey designed to assess general IT use, to identify users of a fully functional EMR system, and to evaluate users’ EMR implementation experience. Survey questions were developed after considering current IT policies in BC and Canada, conducting a systematic literature review, and consulting with experts. Criteria were also established for a fully functional EMR system. Data were collected using online and paper forms and analyzed using SPSS software.
Results: 928 members of the BC College of Physicians and Surgeons completed the survey. Survey findings indicated that 33.3% of respondents accessed information from an EMR during a patient visit and identified some key barriers and incentives for IT and EMR adoption. Survey findings also indicated that 35% of eligible BC doctors planned to register with PITO for EMR implementation funding and support in 2008. Important factors found to advance EMR functionality were physician user type, whether paper charts were retrieved, and overall satisfaction with the EMR used.
Conclusions: The use of fully functional EMR systems for daily patient care in outpatient settings remains low in BC. However, study results suggest that physicians are now ready for widespread EMR adoption through PITO. Successful EMR adoption will require comprehensive implementation assistance, ongoing funding, respect for the autonomy of physicians as independent medical practitioners, and incentives to increase their level of EMR competency. The effectiveness of IT and EMRs can ultimately be expected to achieve evidence-based quality of care improvements.
Although computers are widely used in medical offices throughout the province, few physicians use an EMR to record and view information during a patient encounter.
The integration of information technology (IT) in general and electronic medical records (EMRs) in particular has been identified as an essential component of health care reform in Canada.[1,2] EMRs have been shown to improve quality of care by:
• Increasing patient safety through reducing medication errors.[3]
• Increasing the efficiency of care through reducing duplicate testing.[4]
• Improving the effectiveness of care by assisting physicians using clinical decision support systems (CDSS).[5,6]
• Improving the timeliness of care through faster access to clinical information at the point of care.[7]
• Improving health delivery analysis through more efficient outcome assessment, research, and audit to inform decision making both at the individual practice level and across the health system.[8]
With increasing recognition that all levels of government must work collaboratively to set standards, leverage regional capabilities, and build capacity to enable IT in health care delivery, Canada Health Infoway was established in 2001. The stated goal of this independent, nonprofit organization, whose members are Canada’s federal, provincial, and territorial deputy ministers of health, is to facilitate the development of the IT infrastructure required for the creation of a pan-Canadian patient electronic health record.[9]
Physician organizations, including the Canadian Medical Association and the British Columbia Medical Association, have developed policy statements and recommendations that address how the physician community should contribute to the shaping of the IT agenda in this country, as federal, provincial, territorial governments, and associated agencies move forward with their investments.[10,11] Electronic or computer-based medical records were identified as a key component of the IT strategies outlined by these physician organizations.
In the negotiated agreement between the BCMA and the provincial government ratified in May 2006, funding for the expansion of information technology was established to assist physicians in the setup and ongoing maintenance of office-based electronic medical record systems. The Physician Information Technology Office (PITO) was formed to administer this funding and to assist with EMR implementation.[12] PITO program offerings have been open to eligible physicians since March 2008.
Several Canadian surveys of physician IT and EMR use have been conducted since 2003. Studies conducted in 2004 and 2007 by the National Physician Survey contained several questions on technology use in practice.[13,14] The 2003 BCMA IT survey and 2005 CMA/Infoway survey were specifically IT focused, but were not designed to obtain any detailed data on existing EMR users.[15,16] The primary objective of the survey described in this article was to update our understanding of the status of IT use in BC, with a specific focus on EMR use among practitioners. We sought to do this by addressing the following questions:
• What is the current level of IT use at the point of care?
• What are the current barriers and incentives for adopting an EMR system?
• How ready are physicians for EMR adoption?
• How are EMRs in current outpatient offices being used in practice?
• What was the implementation experience for clinics with existing EMRs?
A more detailed analysis and discussion of the results summarized here can be accessed at http://web.his.uvic.ca/Research/HTG/library/JournalPublications.php.
Survey development
The survey was developed after investigators reviewed current IT policy directions of the federal and provincial governments, paying special attention to the BC scene. Other similar survey reports were reviewed, including the 2003 BCMA IT survey. Reference articles that presented conceptual frameworks for understanding barriers and incentives for information technology adoption[17,18] were used to compile a list for the relevant section of the survey. A systematic literature review was undertaken with other participants in a health informatics training program[19] to identify EMR implementation success factors in primary health care. Factors associated with success in EMR implementations were identified. A meta framework that organized these factors temporally and according to complex social and technical interactions during an EMR implementation was formulated and used to develop the questions in the implementation best practices section of the survey.[20] Local and national experts in medical informatics, organizational management, and health policy analysis helped finalize the content of the survey.
One of the objectives of the survey was to determine the current level of physician outpatient EMR use. Because there is no accepted standard for what constitutes a fully functional EMR system, a minimum but practical set of qualifying EMR functions was developed from a review of the common features in currently available software products, definitions in the literature, criteria from PITO’s early adopter program, and consultation with experts in the field. A fully functional EMR system was defined as a hardware and software system capable of providing a medical practice with the following:
• Appointment scheduling.
• Electronic billing.
• A system to receive, view, and record patient data electronically.
• A system to convert and integrate paper documents.
• A system that allows for communication between physicians and office staff.
• At least one built-in clinical/practice tool.
Survey administration
All 8884 members of the College of Physicians and Surgeons of BC as of September 2007 were invited by fax or e-mail to voluntarily and anonymously complete the survey, either on paper or by logging on to a web survey page. The survey was available from 2 October 2007 to 14 December 2007. Respondents were first asked to indicate whether a full EMR system using the criteria developed for the survey was available at their main practice setting, then directed to either an EMR “user” or “nonuser” survey. Both surveys contained common questions on demographics, IT use, adoption barriers/incentives, privacy, and readiness for participation in PITO. The user survey asked additional questions on the EMR system used and implementation processes.
Statistical analysis
Data collected from online and paper forms were compiled in SPSS v16.0 for further analysis. Chi-square tests were used to compare EMR users’ characteristics with those of nonusers, determine the significance of differences between user profiles and EMR functions, and compare survey demographic data with external references that included the current membership database from the BC results of the 2007 National Physician Survey[14] and physician geographic distribution statistics from the BC Ministry of Health.[21] Logistic regression analysis was used for testing any significant relationships between each IT tool (dependent variable) and respondent characteristics (independent variables). The Mann-Whitney U test was used for comparing ranking of barriers and incentives among different user groups if there were two subgroups; otherwise, the Kruskal-Wallis test was used.
Results
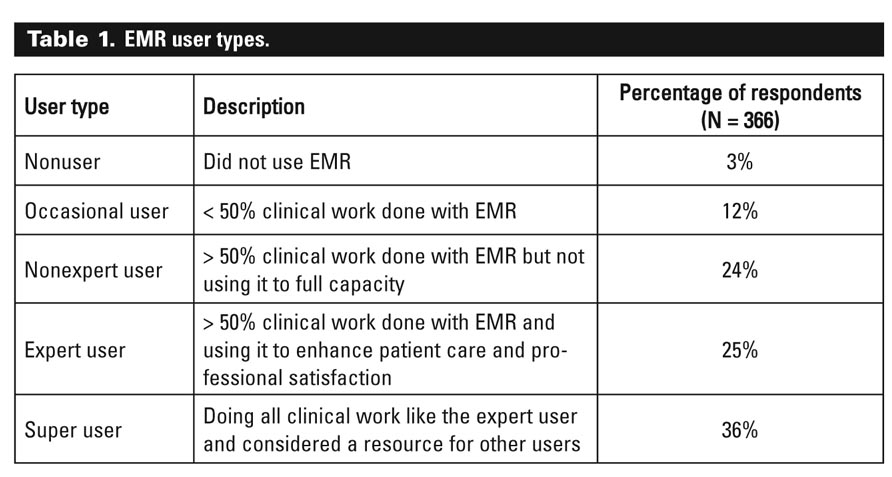
From invitations sent to 8884 BC physicians, a total of 928 surveys were completed, yielding a response rate of 10.45%; 418 respondents completed the EMR user survey and 510 completed the nonuser survey. EMR users were further grouped according to five user types including “occasional users” and “super users” (Table 1). There were no significant differences in the characteristics of the total respondent pool (user vs nonuser) when compared with corresponding external reference demographic data. However, significantly more user respondents had been in practice 11 to 20 years in mainly outpatient settings.
{kind=link}
Although general IT use at the main practice setting was common (Figure 1), only 33.3% of survey respondents indicated that they accessed information from an EMR during a patient visit. EMR users were more likely than nonusers to rely on general IT tools (73% vs 62%), and responses suggested that 35% of eligible BC doctors (approximately 2500) could be expected to register with PITO for EMR implementation funding and support in 2008.
The top three barriers to EMR adoption identified by respondents were cost, time and effort to change, and the lack of a suitable EMR solution. The top three incentives identified were improved patient information access, improved quality of patient care, and increased savings from practice efficiency gains. The main concerns about privacy and security involved the possibility of patient information being accessed by unauthorized users and unauthorized use of data by third parties.
Irrespective of current EMR use, 34% of survey respondents did not agree with and 23% were unsure about the development and implementation of a pan-Canadian interoperable electronic health record. Major concerns were privacy and security, the prohibitive cost, the technical challenge, and jurisdictional political issues.
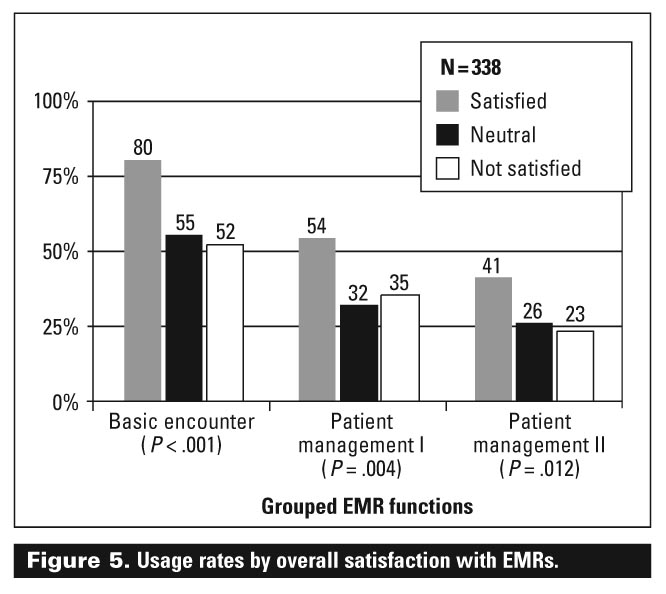
The majority of EMR users (86%) were found to have used their EMR system for more than 1 year, with 47% for more than 3 years. The EMR functions used (Table 2) included a group of “basic encounter” functions, such as accessing patient information and entering notes, and two levels of “patient management” functions, such as completing forms (level I) and searching a database (level II).
{kind=link}
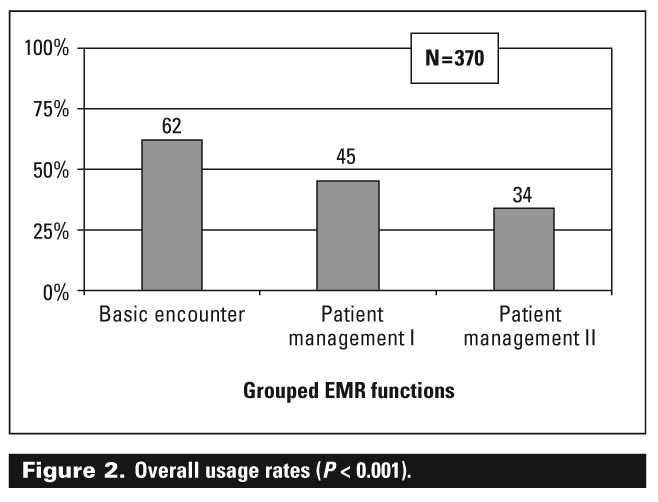
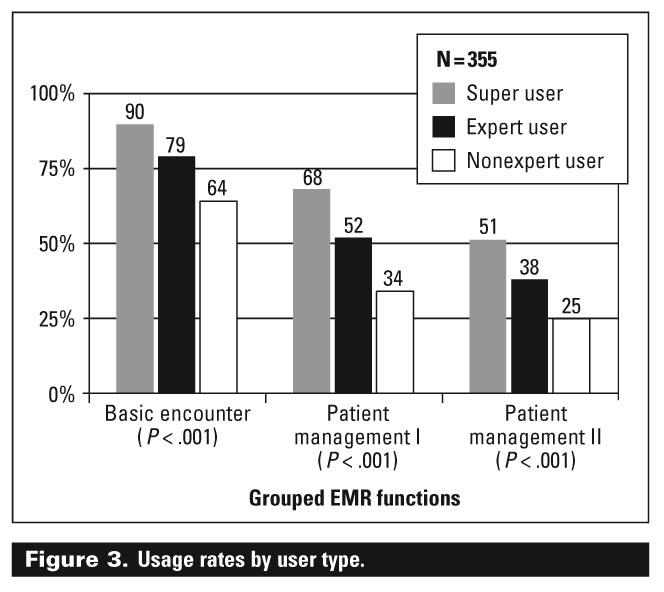
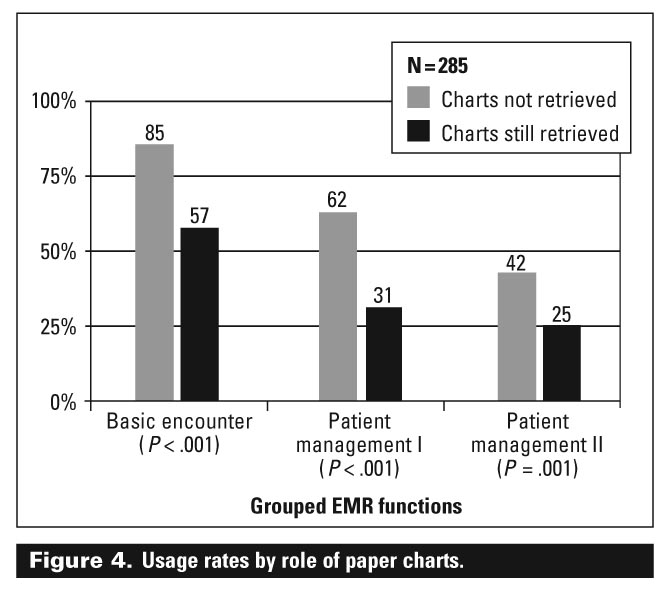
When average physician usage rates for each group of EMR functions were compared, there was a statistically significant decline in overall use from basic encounter (62%) to patient management level I (45%) to patient management level II (34%) (Figure 2). This pattern was also observed within each group of EMR functions when usage rates were compared for different types of EMR users (Figure 3), the role of paper charts in the practice (Figure 4), and overall user satisfaction (Figure 5). However, there were no statistically significant differences in the average usage rates for each group of EMR functions based on the time since an EMR system was implemented (Figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The majority of users (70%) indicated that even though implementing an EMR had a negative impact on practice revenue and expenses, it had an overall positive impact on patient care quality, practice workflows (logistics of patient scheduling, office visits, referrals, follow-up, etc.), and business processes (billing, staffing, and administrative procedures). The most important factors for implementation success, identified by more than 70% of respondents, were the presence of a physician champion, a clearly developed vision, vendor assistance, and an established disaster recovery plan.
The results of this study show that in BC there is widespread use of IT at the point of care. However, only a minority of GPs and specialists use an EMR to record and view information during a patient encounter, a fact consistent with findings from international and Canadian surveys done in the last 4 years.[13,14,16,22,23] This minority of early adopter EMR users is distributed across all regions of the province. The typical early adopter in BC is a physician leader and super user who was able, either independently or in collaboration with several like-minded colleagues in a group setting, to develop a clear vision for an EMR-enabled practice and to find a reliable vendor who provided suitable software, implementation assistance, and disaster recovery support. The implementation period was by necessity short, taking less than 3 months because time was likely at a premium for physicians who were also engaged in busy clinical practice.
Closer analysis of EMR functions used by early adopters in patient care showed that the level of use was low. Therefore, although the majority of users described a successful EMR implementation, optimal use of EMR functions that would be expected to produce evidence-based benefits and practice quality improvement[24] were not seen in this study. There was no correlation of increasing optimal EMR use with the length of time since implementation. However, important factors that advanced the level of EMR functionality were user type, the extent to which paper charts were no longer retrieved, and overall satisfaction with EMRs.
Implementation requirements
EMR implementation requires not only a large up-front financial investment, but also the introduction of new technology and management of the associated workflow changes for physicians and office staff. Consistent with the findings in this study, significant barriers to widespread adoption have been identified in the literature.[25-27] These barriers include the lack of external funding for high start-up and maintenance costs, EMR vendor volatility, initial practice disruption, lack of short-term return on investment with benefits instead accruing to insurers or payers, concerns regarding privacy and security, and the medical community’s collective culture that often views EMRs as a threat to professional autonomy. Experience in other countries, such as the UK, Scandinavia (Denmark, Sweden, Norway), Australia, and New Zealand,[28] shows that a funding and support program aimed at the average physician EMR adopter increases the likelihood of successful implementation. In BC, this kind of program is now available through PITO, which aims to promote widespread use of EMRs by:
• Validating the leadership role that physicians play in any EMR implementation.
• Providing strong preimplementation support with emphasis on practice and workflow assessment, software and hardware selection, and assistance in privacy impact assessment.
• Identifying EMR vendors with comprehensive implementation support services.
An EMR implementation is actually an ongoing process that doesn’t stop after the “go-live” date. Adoption of high-level EMR functions is critical to ensure that the recognized patient care quality improvements cited in the literature are realized. These functions include a prescription writer and drug interaction alert module, chronic disease management functions (flow sheet, registry, chronic disease management toolkit integration), guideline-based clinical decision support, and integration with other information systems. As BC physicians begin to participate individually or in communities of practice in the PITO program, additional support and incentives will be needed to promote postimplementation training for both physicians and staff that increase the level of EMR competency and advance user level. High-level EMR functionality is an important enabler of incentive-driven practice change, as seen in the BC primary care Practice Support Program.[29] Long-term funding to promote and support advanced use of installed EMR systems is currently not part of the PITO program.
Study limitations
A recognized limitation of this study, consistent with all survey methodologies, is an upward bias on the results. Physicians already using EMRs or very interested in EMRs were more likely to respond to the survey than nonusers. Over 50% of survey respondents were, in fact, EMR users, an unusually high number when respondents were compared with the general physician population. However, a recent retrospective analysis of a large IT survey of physicians failed to detect significant response bias and suggested that similar surveys of physicians, even with a lower than expected response rate, may still be valid.[30] Despite this study’s explicit attempt to define a fully functional EMR system, respondents with a system that did not meet the criteria may have qualified themselves and proceeded with the EMR user survey. Both biases would have played a part in over-inflating the determination of the overall EMR usage rate in this study.
The limitations of survey methodology also make it difficult to accurately assess complex processes such as EMR implementation or tease out nuances of EMR use in practice. Early adopters who personally invested in their own EMR systems were potentially more likely to respond positively to questions relating to success factors in EMR implementation and overestimate their use of EMR functions. As there are no accepted standard definitions of various EMR functions, survey questions—which by necessity can only briefly describe a particular EMR function—may be interpreted differently by different respondents, depending on the particular software product used. More than 50% of respondents implemented their EMR system 3 or more years ago and may not have accurately recalled details of their implementation experience.
As the number of provincial IT support programs increase and more physicians decide to incorporate EMRs in their practices, there will be greater opportunity to conduct more comprehensive studies. Richer data can be obtained from field studies and immediate postimplementation reviews. A standardized and accepted set of criteria for a fully functional EMR system will be critical for facilitating comparisons between studies. Prospective studies designed to monitor the level of EMR use following adoption will also help determine whether the current evidence-based benefits for improved quality of care can be further substantiated.
Conclusions
EMR implementation is a process that not only requires strong preimplementation support and EMR vendors who provide comprehensive implementation assistance, but the ongoing promotion of high-level EMR functions to ensure that evidence-based quality of care improvements are realized. Despite widespread use of IT in physician offices in BC, the use of fully functional EMR systems for daily patient care in outpatient settings remains low. Many physicians remain skeptical, given the complex nature of EMR implementation and the broader implications for privacy and confidentiality. However, now that conditions known to facilitate the widespread adoption of EMRs are present in BC with PITO as part of an overarching e-health strategy for the province, this should change. In order to accelerate EMR adoption, BC doctors need sustained funding, up-to-date information on government IT agendas, implementation assistance, and user support—all while respecting their autonomy as independent medical practitioners.
Funding for this study was provided by the Physician Information Technology Office (PITO), eHealth Strategy Office, Faculty of Medicine, University of British Columbia, and the CIHR Health Informatics PhD-Postdoc Strategic Training Program. The authors would like to acknowledge the leadership and support of the following people, who all ensured the successful completion of this study: Ms Ju Yang, School of Health Information Science, University of Victoria; Dr Kendall Ho and Ms Celine Cressman, eHealth Strategy Office, Faculty of Medicine, University of British Columbia; Mr Tunde Olatunbosun, Division of Continuing Professional Development, Faculty of Medicine, University of British Columbia; Dr Denise Buote, Arbor Educational Clinical Consulting Inc.; Dr Alexandra Tcheremenska-Greenhill, British Columbia Medical Association; Mr Jeremy Smith, Physician Information Technology Office.
The study was funded in part by the Physician Information Technology Office (PITO) in the form of an unrestricted research grant. Dr Lai received consulting fees (BCMA GP sessional) from PITO from August 2006 to November 2006 and in January 2007 as a member of a physician advisory group for EMR requirements review, and from April 2008 to the present as a local physician champion to support the PITO Implementation and Transition Support Program.
References
1. Romanow R. Building on Values: The Future of Health Care in Canada—Final Report. Ottawa: Commission on the Future of Health in Canada; 2002.
2. Health Council of Canada. Health Care Renewal in Canada, Clearing the Road to Quality. Annual Report to Canadians 2005. Toronto: HCC; 2006.
3. Tamblyn R, Huang A, Perreault R, et al. The medical office of the 21st century (MOXXI): Effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care. CMAJ 2003;169:549-556.
4. Mekhjian H, Kumar R, Kuehn L, et al. Immediate benefits realized following implementation of physician order entry at an academic medical center. J Am Med Inform Assoc 2002;9:529-539.
5. Ornstein S, Garr D, Jenkins R, et al. Computer-generated physician and patient reminders. Tools to improve population adherence to selected preventive services. J Fam Pract 1991;32:82-90.
6. Garg A, Adhikari N, McDonald H, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes. JAMA 2005;293:1223-1238.
7. Forsythe D, Buchanan B, Osheroff J, et al. Expanding the concept of medical information: An observational study of physicians’ information needs. Comput Biomed Res 1992;25:181-200.
8. Nordyke R, Kulikowski C. An informatics-based chronic disease practice: Case study of a 35-year computer-based longitudinal record system. J Am Med Inform Assoc 1998;5:88-103.
9. Canada Health Infoway. Creating Healthy Connections. Annual Report 2004–05. www2.infoway-inforoute.ca/Documents/Annual Report 04-05 EN.pdf (accessed 12 February 2009).
10. Canadian Medical Association Health Information Technology Committee. Shaping a pan-Canadian e-health environment for physicians and patients. A discussion paper. 2002. www.cma.ca/multimedia/staticContent/HTML/N0/l2/HIT/pdf/e-health-discussi... (accessed 12 February 2009).
11. British Columbia Medical Association. Getting IT right: Patient-centred information technology. A discussion paper by BC’s Physicians. 2004. www.bcma.org/files/GettingITRight.pdf (accessed 10 Mar 2009).
12. Physician Information Technology Office. www.pito.bc.ca/default.htm (accessed 1 October 2008).
13. College of Family Physicians of Canada, Canadian Medical Association, Royal College of Physicians and Surgeons of Canada. 2004 National Physician Survey. www.nationalphysiciansurvey.ca/nps/2004_Survey/2004nps-e.asp (accessed 17 September 2008).
14. College of Family Physicians of Canada, Canadian Medical Association, Royal College of Physicians and Surgeons of Canada. 2007 National Physician Survey. www.nationalphysiciansurvey.ca/nps/2007_Survey/2007nps-e.asp (accessed 17 September 2008).
15. British Columbia Medical Association Information Policy Group. BCMA physician survey on IT. 2004.
16. Canadian Medical Association. Results of the CMA 2002 physician resource questionnaire. www.cmaj.ca/cgi/content/full/167/5/521/DC1 (accessed on 17 September 2008).
17. Valdes I, Kibbe D, Tolleson G, et al. Barriers to proliferation of electronic medical records. Inform Prim Care 2004;12:3-9.
18. Johnson K. Barriers that impede the adoption of pediatric information technology. Arch Pediatr Adolesc Med 2001;155:1374-1379.
19. The CIHR Health Informatics PhD/Postdoc Strategic Training Program. http://web.his.uvic.ca/chpstp/ (accessed 9 February 2009).
20. Keshavjee K, Bosomworth J, Copen J, et al. Best practices in EMR implementation: A systematic review. AMIA Annu Symp Proc 2006:982.
21. Ministry of Health Services. MSP Information Resource Manual Fee-for-service Payment Statistics 2006/2007. Victoria, BC: Government of British Columbia.
22. Schoen C, Osborn R, Huynh P, et al. The Commonwealth Fund 2006 International Health Policy Survey of Primary Care Physicians in Seven Countries. New York: Commonwealth Fund; 2006.
23. DesRoches C, Campbell E, Rao S, et al. Electronic health records in ambulatory care—A national survey of physicians. N Engl J Med 2008;359:50-60.
24. Litvin CB, Ornstein SM, Anthony W, et al. Quality improvement using electronic medical records: A case study of a high-performing practice. Top Health Inf Manage 2001;22:59-64.
25. Sobol M, Alverson M, Lei D. Barriers to the adoption of computerized technology in health care systems. Top Health Inf Manage 1999;19:1-19.
26. Tonnesen A, LeMaistre A, Tucker D. Electronic medical record implementation barriers encountered during implementation. Proc AMIA Symp 1999:624-626.
27. Anderson J. Social, ethical and legal barriers to e-health. Int J Med Inform 2007;76:480-483.
28. Protti D. Comparison of information technology in general practice in 10 countries. Healthc Q 2007;10:107-116.
29. Practice Support Program. www.impactbc.ca/practicesupport (accessed 1 October 2008).
30. Menachemi N, Hikmet N, Stutzman M, et al. Investigating response bias in an information technology survey of physicians. J Med Syst 2006;30:277-282.
Dr Lai is a clinical associate professor in the Department of Family Practice at the University of British Columbia. Dr Lau is an associate professor at the School of Health Information Science, University of Victoria. Dr Shaw is research chair, Health Informatics, at the University of Alberta.