By: Alana Godin Afsaneh Moradi
The value of data: Identifying patient and community needs to inform primary care networks
Issue: BCMJ,
vol. 61, No. 6, July August 2019,
Pages 261-262 Family Practice Services Committee
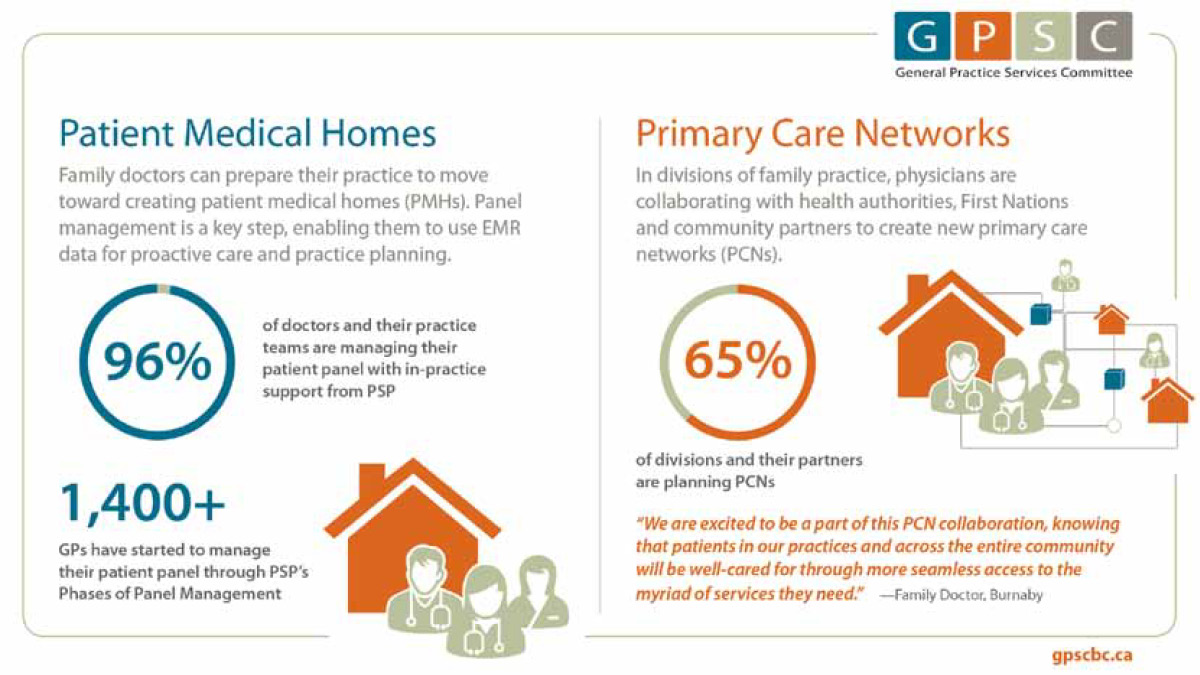
BC’s health care system is undergoing changes that will connect more patients with primary care and enable physicians to help patients access additional services and support. This involves increasing team-based health care through the creation of patient medical homes (PMHs) in family practices and forming primary care networks (PCNs) in communities that support longitudinal care provided by PMHs. As of June 2019, nine divisions of family practice have announced plans to form PCNs in their communities. An additional 16 divisions are planning to undertake the PCN expression of interest process in the coming months.
Data from physician practices are key to taking a practice to the next level as a PMH and enabling participation in team-based care and PCNs. Strong EMR data help identify how many patients are in the practice, what conditions those patients have, and the kinds of in-practice and team-based supports (like allied health providers) that can help provide proactive care for these patients. This in turn helps divisions understand the needs of patient populations and the broader communities as they plan PCNs.
To contribute accurate, up-to-date data to inform the PCN planning process, physicians can adopt PMH attributes in their practice and undertake the General Practice Services Committee’s Phases of Panel Management.[1] As of May 2019, more than 1300 doctors around the province were involved in this work. Updating patient data through the Phases of Panel Management also benefits physicians and their patients in a number of ways:
- Identifying active versus inactive patients. One physician who is now proactively managing his patient panel through support from the Practice Support Program assessed his panel and discovered he had 1100 active patients (he had expected closer to 2000 as he had taken over a full-sized practice). This data prompted him to open his practice to new patients.[2]
- Identifying services and team members appropriately to best serve patients. Panel data enable physicians to advocate for appropriate resources to meet patients’ needs, such as allied care providers.
- Using aggregated data to plan patient supports and services in the community as a whole. Physicians can choose to share their aggregated panel data with divisions to identify the broader needs of the community, inform the division’s PCN expression of interest process, and help budget for the supports patients need.
- Providing proactive and preventive patient care. With clean EMR data, doctors can pull lists of patients with specific needs and organize preventive screening and proactive processes for disease management. One physician reported that panel management enabled him to streamline his immunization registry and to more than double the number of patients who had a recorded flu vaccine status within 2 months.[2]
- Simplifying workflows to help with patient care, such as referral callbacks, reports, and accurate resources. Based on EMR data, Practice Support Program regional support teams can provide tailored supports to help physicians improve workflow efficiencies in specific areas, enabling them to focus on patient care.
- Keeping track of patient activities to bill effectively for services provided (e.g., complex care), earning extra revenue for the practice. In some cases, this extra resource may help to increase team-based supports in a practice.
- Improving patients’ experiences of care. Panel management has been shown to increase continuity of care, meaning that the patient’s experience of care is more coherent, consistent, and connected. This process is associated with improved patient-provider relationships, better coordinated care, and increased preventive and proactive care.
Supports for family doctors
The GPSC supports physicians to update and manage their patient data in a number of ways. Regional support teams, panel assistants,* and remote EMR services* are available through the Practice Support Program to help physicians clean up their data, and the Panel Development Incentive compensates eligible family doctors for their time and effort to develop and manage their panels. The Doctors Technology Office (DTO) provides EMR supports as well. See the list of GPSC and DTO supports, along with links to additional information [Table].
More information on primary care networks
To learn more about primary care networks, visit the GPSC website (www.gpscbc.ca/what-we-do/system-change/primary-care-networks) and contact your local division of family practice to find out how to contribute to PCN planning and implementation in your community.
—Alana GodinDirector, Community Practice and Quality, Community Practice, Quality and Integration Department
—Afsaneh MoradiDirector, Community Partnership and Integration
* Panel assistants and remote EMR services are currently only available in PCN communities.
hidden
This article is the opinion of the GPSC and has not been peer reviewed by the BCMJ Editorial Board.
References
1. General Practice Services Committee. Professional development. Panel management. Accessed 22 May 2019. www.gpscbc.ca/what-we-do/professional-development/psp/panel-management.
2. General Practice Services Committee. Our Impact. Proactive panel management improves practice efficiency in Cowichan Valley. Accessed 23 May 2019. www.gpscbc.ca/our-impact/practice-support/proactive-panel-management-improves-practice-efficiency-cowichan-valley.

What is a panel assistant and what is a remote EMR?