By: Fawziah Marra, PharmD Sunny Mak, MSc Mei Chong, MSc David M. Patrick, MD, FRCPC, MHSc
Regional variations in antibiotic consumption in BC
Issue: BCMJ,
No. 10, December 2008,
Pages 576-577 BC Centre for Disease Control
Bacterial resistance to antimicrobial agents has become a major public health threat.[1] Few novel antibiotics have been developed as therapeutic alternatives in the last decade. Because the rate of antibiotic use is a major contributing factor to resistance,[2],[3] surveillance of antibiotic use is becoming an important tool in changing prescription patterns. The European Surveillance of Antimicrobial Consumption (ESAC) project has been collecting data on antibiotic use across European countries since 1997 and demonstrates varied consumption by country.[4] BCCDC has been working with the BC College of Pharmacists to track outpatient consumption of antibiotics.
The overall rate of antibiotic use among outpatients in British Columbia has slowly declined from 18.5 to 16.8 defined daily doses per 1000 inhabitant-days between 1996 and 2007. However, the trend has not been without bumps as use increased from 2004 to 2005 but has largely leveled off since.
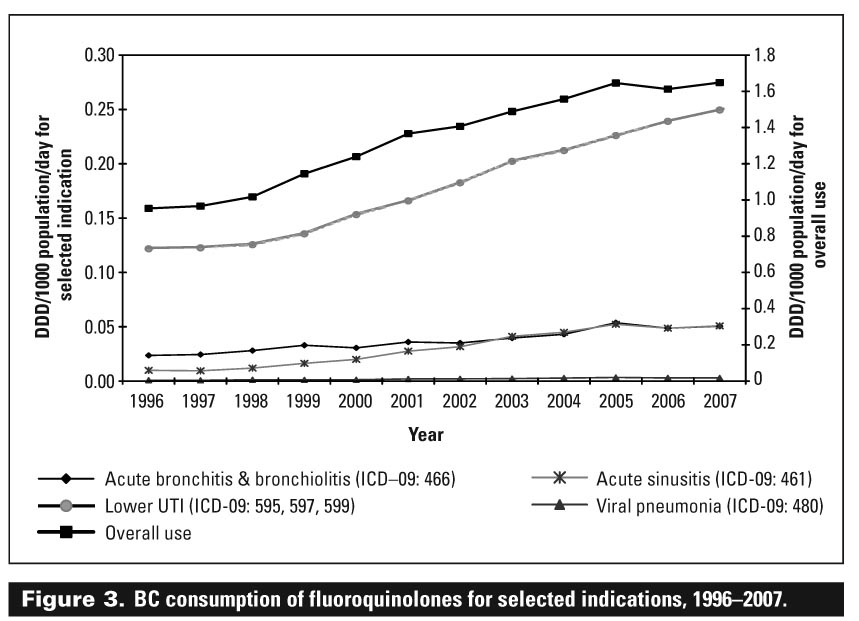
In general, antibiotic consumption rates were higher in the northern and interior regions of the province, although use has declined recently in the northeast [Figure 1]. An evaluation of the specific classes shows that consumption of narrow spectrum agents such as penicillins has plateaued over the last 5 years; tetracyclines and trimethoprim/sulfamethoxazole use have declined significantly, while use of the newer macrolides and fluoroquinolones has increased significantly. When indications for use are examined, macrolides are used commonly for respiratory tract infections while fluoroquinolones are used for urinary tract infections [Figure 2] and [Figure 3].
{kind=link}
{kind=link}
Although we have shown that overall antimicrobial use has decreased, it is apparent that there is a substantial increase in use of broad spectrum agents, particularly the macrolides and newer fluoroquinolones (levofloxacin and moxifloxacin). As such, we need to focus our efforts to reduce inappropriate use of these agents, in particular through:
• Public education about how certain infections do not require antibiotics.
• Reinforcement of basic infection control practices in the community, such as hand washing.
• Reinforcement among physicians and pharmacists that many classes of infection do not require antibiotics to resolve and that first line (e.g., simple beta-lactam) antibiotics are an appropriate first step in managing many community-acquired infections.
References
1. Wise R, Hart T, Cars O, et al. Antimicrobial resistance. BMJ 1998;317:609-610.
2. Bergman H, Huikko S, Pihlajamaki M, et al. Effect of macrolide consumption on erythromycin resistance in Streptococcus pyogenes in Finland in 1997–2001. Clin Infect Dis 2004;38:1251-1256.
3. Bronzwaer SL, Cars O, Buchholz U, et al. A European study on the relationship between antimicrobial use and antimicrobial resistance. Emerg Infect Dis 2002;8:278-282.
4. Goossens H, Ferech M, Vander Stichele R, et al. The ESAC Project Group. Outpatient antibiotic use in Europe and the association with resistance: A cross-national database study. Lancet 2005;365:579-587.
hidden
Dr Marra is an associate professor in the Faculty of Pharmaceutical Sciences at the University of British Columbia and director of Pharmacy and Vaccine Services at the BC Centre for Disease Control. Mr. Mak is the senior medical geographer at the BCCDC. Ms Chong is a biostatician at the BCCDC. Dr Patrick is the director of Epidemiology Services at the BCCDC.