Whiplash: The role of imaging—To X-ray or not?
Issue: BCMJ,
vol. 44, No. 5, June 2002,
Pages 248-251 Clinical Articles
Recent studies on the role of radiography in defining whiplash injuries help physicians identify the patient with an unrecognized, unstable injury of the cervical spine and the associated risk of a devastating or life-threatening injury to the spinal cord. The “shot-gun” approach of requesting radiographs on every patient with a whiplash injury is being modified as we understand the subgroups of patients with whiplash injuries who can be reliably predicted to have normal radiographs.
A patient involved in a simple rear-end collision who later presents with the complaint of neck pain may not require radiographic evaluation, but if there is any suspicion of a fracture or instability, radiography must be carried out.
The indiscriminate use of radiographs has been primarily driven by the ever-present concern of cervical spine stability.[1-3] An estimated 200 000 radiographs of the cervical spine are carried out annually in Canada on patients who have been injured through blunt or secondary trauma to the neck. Avoiding radiographs for those patients where the results are predicted to be normal translates to significant savings to our medical system and a reduction in the exposure of patients to ionizing radiation.[1,4-6]
Some authorities still recommend the routine inclusion of plain film radiography for any case where trauma to the neck occurs and the clinical finding of midline posterior neck tenderness is present.[1,3] It is recognized that patients sustaining a cervical injury (whiplash) from a rear-end motor vehicle collision may be seen in a variety of settings including emergency departments, family doctors’ offices, and clinics. Simply stated, radiography is indicated if the possibility of a fracture exists.[2]
Initiatives are under way in Canada and the United States to help identify the groups of patients with blunt trauma (whiplash associated disorders, WAD I and less commonly WAD II; see the Table in the article "Incidence of whiplash-associated disorder" for a definition) where the history and physical examination can clearly exclude significant pathology.
Decision rules regarding the need for radiographs are being validated that will allow selective ordering of imaging studies. The NEXUS study, a decision rule cervical spine radiograph study, has received wide interest in the United States.[1] The CCC (Canadian C-Spine) study under the direction of Ian Stiell at the University of Ottawa is in the advanced stages of validation in Canada, with a current enrollment of 14 000 patients. Investigators in the CCC study are currently completing a multicentre investigation in Canadian urban teaching hospitals whereby a set of low-risk factors can predict the selection of patients who can then be allowed a supervised assessment of range of motion. The next step in the process of validation will be to ensure that these low-risk criteria can also be applied in the settings of community hospitals and primary clinics. Then, when an evaluation occurs in a broad range of settings given the identified low-risk factors, it is postulated that the ability to rotate the neck may reliably predict all individuals who do not require radiography.
Radiography is recommended when high-risk factors are present, such as age greater than 65 years, a defined dangerous mechanism (see the Table), or any report of a sensory abnormality or focal neurologic deficit in the extremities. Plain film imaging is also recommended in the setting where examination of the neck is unreliable, such as with distracting painful injuries elsewhere, altered level of consciousness, or evidence of facial or external head injury. In addition, radiographic evaluation is recommended for any patient where active neck rotation cannot be completed by the patient in the defined manner.
Though it must be emphasized that these features have yet to be validated, a patient involved in a simple rear-end motor vehicle collision who later presents with the complaint of neck pain may not require radiographic evaluation. However, if there is any suspicion of a fracture or instability, clinical judgment is still the overriding principle and radiography must be carried out while ensuring immobilization of the cervical spine.
Radiographs may show a non-specific loss of normal lordosis or straightening (Figure 1) but alone do not indicate a specific diagnosis of whiplash.[2] Young people in particular can often reverse the lordotic curve with the simple instructions to sit tall and tuck in their chin. If the lordosis reversal is accompanied by swelling along the anterior longitudinal ligament, significant regional trauma may be present. Radiographs help to rule out fractures or malalignment of the cervical spine. Soft-tissue swelling may be evident, and this too requires further evaluation by additional views or alternate modalities to rule out a significant fracture or instability.
Plain film radiography may also reveal the degenerative changes common to older people. A variety of radiographic features indicate pre-existing degenerative processes, including:
• Osteophyte formation.
• Vertebral body malalignment.
• Loss of vertebral body height.
• Calcification of the anterior longitudinal ligament.[7]
Sclerosis of bony margins and the presence of widespread degenerative change can assist in the differentiation of acute from chronic processes. However, identification of an acute injury in the setting of degenerative changes can be challenging. CT scanning can be particularly useful when confronting this dilemma and can greatly assist in the differentiation between pre-existing changes and new abnormalities.
A detailed description of the radiographic interpretation of the cervical spine is beyond the scope of this review, but excellent references are available.[2,3] The current standard set of radiographs undertaken in the setting of a possible fracture or unstable cervical spine injury consist of a standard three-part series of X-rays. These include a lateral view with visualization of the superior aspect of the vertebral body of T-1 (Figure 1), an anteroposterior (AP) view (Figure 2), and an open-mouth or odontoid view (Figure 3). Some centres recommend the inclusion of left and right oblique projections, and many centres include a swimmer’s view for better visualization of T-1 (Figure 4).
These films are carried out while employing the following strict spinal precautions: from the time of presentation until the completion of the radiographic evaluation, the patient lies on a long spine board with a hard, appropriately sized collar and sand bags adjacent to each side of the head. These precautions prevent movement and minimize the risk of neuronal injury should a significant or unstable injury exist.
Ancillary studies that may be indicated include flexion/extension views, pillar views, and special imaging modalities. Flexion/extension views may be requested when no significant fracture or dislocation is evident on plain film radiography or there is no clinically evident neuronal injury, yet disruption of the anterior longitudinal ligament is suggested on clinical or radiographic grounds. Significant disc space widening or soft-tissue swelling anterior to the spinal column may indicate the need for this additional series of radiographs.
Computed imaging can help clarify an abnormality on plain film to identify a fracture or unstable segment. CT scanning is not considered part of the radiographic work-up of a patient with a simple rear-end motor vehicle collision related neck injury.[2] It is recognized that this form of imaging can be very useful in specific settings, but for the vast majority of patients with whiplash injuries, it is not required and is not readily available.
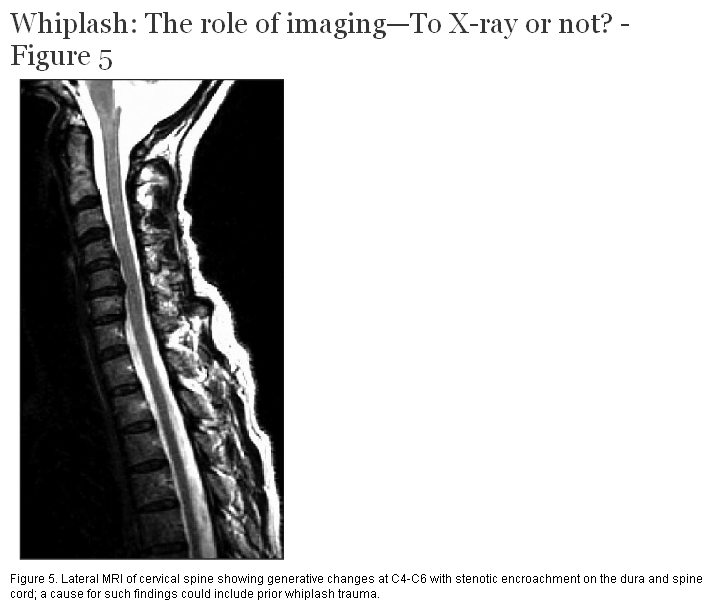
Does magnetic resonance imaging (MRI) identify the soft-tissue trauma that could correlate with whiplash injuries? Thus far, though reports have been inconsistent, the abnormalities detected have a poor correlation with actual injury patterns and symptoms. Abnormalities detected with MRI may be present with or without a history of a cervical spine type injury, and the presence, when detected, is therefore of questionable significance (Figure 5). MRI is also not considered as part of the initial evaluation of patients with rear-end motor vehicle collision injuries to the cervical spine who have normal radiographs and no evidence of a neuronal injury.[8,9]
Nuclear medicine scans have also been studied in an attempt to correlate structural abnormalities to specific symptoms in patients with neck pain following a rear-end motor vehicle collision. A study of this nature is currently underway in the Department of Emergency Medicine at Vancouver Hospital. Thus far, no specific correlation has been made, yet this modality may hold some promise in helping us understand the nature of whiplash.
Plain film radiography remains the imaging modality of choice. CT scanning and MRI may be indicated for patients with chronic pain syndromes to evaluate the cervical spinal canal for the presence of disc degeneration, nerve root or cord compression, and the need for surgical intervention. These investigations may be indicated in patients with symptoms either in association with or unrelated to any history of a motor vehicle collision.[10]
The future validation of decision rules will give us a strong tool by which we can safely and reliably change our practice. The number of patients that are expected to be enrolled in the CCC study by the time of completion is estimated at 24 000. Validation of Phase II of the rules in the study hospitals is close to completion and is expected in November 2002. The next important step, Phase III, is the anticipated validation of the rules in community hospital and clinic settings. This stage of the process is expected to extend until 2004, when the project will be completed.
For now, any patient who presents with neck pain and has midline cervical spine tenderness in the posterior aspect of the neck as new features following a motor vehicle collision will generally have a series of plain films in order to exclude a cervical fracture.
The recent availability of digital imaging, with its inherent ease of information transmission, will allow for imaging in rural and remote settings with transmission of images for definitive evaluation at expert centres. This will offer the ability to interpret and suggest strategies for intervention at a site distant from the setting where initial evaluation is taking place.
Digital electronic image transfer is included as one of a number of promising applications within the rapidly advancing field of telemedicine. The availability of appropriate and timely reassurance, or alternatively, the recommendation for transfer for definitive care at a tertiary centre, will have a significant impact on the quality of care in remote facilities. Both decision rule validation and digital image transfer will soon be at hand. These initiatives have the potential to offer us real progress in our ability to treat our patients safely and reliably.
None declared.
Table. Risk factors in patients with a purported neck trauma or neck pain that require radiographs of the cervical spine regardless of clinical presentation.
|
• Any alteration in level of consciousness. |
References
1. Hoffman JR, Mower WM, Wolfson AB, et al. The National Emergency X-Radiography Utilization Study Group. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med 2000;343:94-99. PubMed Abstract Full Text
2. Rosen P, Barkin R. Emergency Medicine Concepts and Clinical Practice. 4th ed. St. Louis, MO: Mosby, 1998:878-885.
3. Tintinalli JE, Kelen GD, Stapczynski JS. Emergency Medicine, A Comprehensive Study Guide. 5th ed. New York, NY: McGraw-Hill, 2000:1792-1800.
4. Stiell IG, Wells GA, Vandemheen K, et al. Variation in emergency department use of cervical spine radiography for alert, stable trauma patients. CMAJ 1997;156:1537-1544. PubMed Abstract Full Text
5. Beir V. Committee on the Biological Effects of Ionizing Radiations: Health Effects of Exposure to Low Levels of Ionizing Radiation. Washington, DC: National Academy Press, 1990:281.
6. Huda W, Bissesseur K. Effective dose equivalents, HE, in diagnostic radiology. Diagn Radiol Med Phys 1990;17:998-1003. PubMed Abstract
7. Schwartz D, Reisdorff E. Emergency Radiology. New York, NY: McGraw-Hill, 2000:313.
8. Ronnen HR, de Korte PJ, Brink PR, et al. Acute whiplash injury: Is there a role for MR imaging? A retrospective study of 100 patients. Radiology 1996;201:93-96. PubMed Abstract
9. Petterson K, Hildingsson C, Toolanen G, et al. Disc pathology after whiplash injury. A prospective magnetic resonance imaging and clinical investigation. Spine 1997;22:283-287. PubMed Abstract
10. Voyvodic F, Dolinis J, Moore VM, et al. MRI of car occupants with whiplash injury. Neuroradiology 1997;39:35-40. PubMed Abstract
Bruce Fleming, MD, FRCPC
Dr Fleming is an emergency physician and associate head of the Department of Emergency Medicine at Vancouver Hospital, with an additional clinical appointment at the University of British Columbia Hospital in Vancouver.

{kind=link}
{kind=link}