Vertebroplasty: An effective technique in the treatment of osteoporotic and malignant vertebral collapse
Issue: BCMJ,
vol. 44 , No. 10 , December 2002 ,
Pages 530-536 Clinical Articles
Vertebral collapse can have a variety of causes, particularly osteoporosis, metastatic disease, and, less frequently, hemangiomas. Traditional therapy has generally consisted of conservative management in the case of osteoporosis. In selected cases, especially with malignant disease, surgical intervention is used. More recently vertebroplasty, a radiologically guided therapeutic alternative, has been introduced. This technique involves placing a bone biopsy needle into the vertebral body and injecting polymethylmethacrylate cement under fluoroscopic guidance. In the majority of instances the procedure can be performed on a day care basis. This technique has proven successful in providing dramatic and prompt pain relief in most candidates, allowing rapid patient mobilization and preventing further compression of the affected vertebral body.
Vertebroplasty is an extremely safe and readily performed procedure, with most patients experiencing dramatic improvement in their symptoms.
Over the past 10 years vertebroplasty, a radiologically guided therapeutic procedure, has undergone rapid development and adoption throughout the world. This technique consists of injecting polymethylmethacrylate (bone cement) into vertebrae to relieve pain and provide structural reinforcement following compression fracture secondary to a variety of causes.[1-3] This technique was originally pioneered in France in the mid-1980s, principally for treatment of vascular bone lesions such as hemangioma, but it was quickly recognized that metastases and plasmacytomas could also be successfully palliated using this technique.[4-6] Not long afterward, a much larger population of patients with osteoporotic compression fractures were also found to benefit greatly from cement injection.
With the widespread introduction of this technique into North America, patients are increasingly becoming aware of its existence and availability. Numerous web sites (a recent Internet search of the term vertebroplasty patient information turned up 1660 sites) promote and explain the procedure, and patients are increasingly approaching their physicians for access to this treatment.
Vertebral fracture secondary to osteoporosis is the most common clinical situation in which vertebroplasty is used. In Canada it is estimated that 40 000 to 50 000 new compression fractures occur each year, and up to one-third of these patients develop significant debilitating pain that responds incompletely to conservative therapy. As most of these fractures occur in elderly individuals, the impact on lifestyle can be significant and can spell the end of independent existence. If bed rest is required for long periods, patient mobility may be permanently affected or other adverse complications, such as deep vein thrombosis and pulmonary embolus, may ensue.[7] Compression fractures are therefore a significant cause of admissions to nursing homes and geriatric hospital beds. In this era of significant health care cost restraint, this represents an important issue. The introduction of a technique that could reduce the impact of this problem would therefore be welcome.[8]
Conventional conservative therapy uses a combination of bed rest, braces, and analgesics (anti-inflammatory or opiate).[9] For many patients this proves quite satisfactory and they are able to regain mobility after only a brief period of convalescence. In those with persistent severe pain and prolonged bed rest, pneumonia, deep vein thrombosis, or pulmonary embolism may become a threat. Social isolation and/or significant additional strain on families is common.
Pharmacologic therapy, such as vitamin D, calcium, estrogen (and the newer estrogen receptor modulators), fluoride, calcitonin, and bisphosphonates are helpful in promoting bone repair and increasing bone mass, but require long time periods before they have a significant effect. These drugs have a role in decreasing future fractures but are not helpful in the acute and subacute periods after fracture. Many patients find these drugs difficult to tolerate due to their side effects. Surgical alternatives are invasive and involve considerable morbidity and mortality. The poor, fragile bone stock provides a suboptimal framework for anchoring surgical hardware. As other treatment methods may be ineffective, vertebroplasty presents an attractive option providing rapid pain relief and accelerated mobilization.
Patient selection and screening
The cardinal issue in these patients is the presence of back pain centred on, or immediately adjacent to, a diseased vertebral body. Generally it is recommended that patients who have osteoporotic compression fractures have had at least 2 weeks to 4 weeks of conservative therapy without any evidence of significant improvement. Although previous work suggested that chronic fractures (those older than 3 months to 6 months) and patients with more than 65% of a collapse of a vertebral body were not suitable, recent work has clearly indicated that many of these patients can be successfully treated with significant benefit.[10-12]
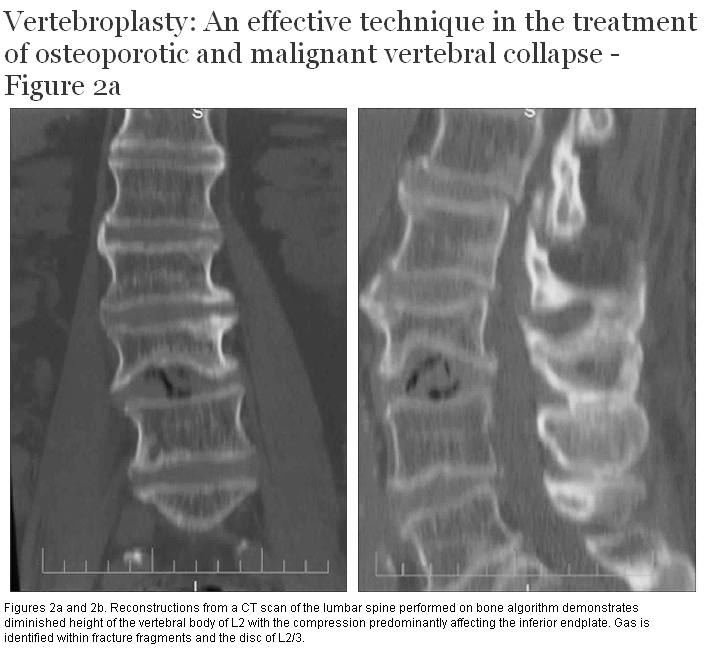
Patients should have both radiographs and cross-sectional imaging (CT or MRI) to assess the severity of the fracture and to assess for areas of cortical disruption or deficiency. The presence of such cortical disruption does not necessarily preclude vertebroplasty, but is important in predicting the most likely site of cement extravasation. Patients with evidence of cord compression, caused either by the presence of a tumor or shifting of bone fragment, are not suitable candidates and are better treated surgically. Cross-sectional imaging also excludes the presence of painful disc protrusion. All patients should have a platelet count and INR, as presence of either thrombocytopenia or coagulopathy is a contraindication.
A variety of techniques have been proposed for performing vertebroplasty. The procedure can generally be performed with conscious sedation, preferably with an anesthetist in attendance. Generous infiltration with 2% lidocaine (Xylocaine) in the soft tissues adjacent to the site of the pedicular puncture is performed, and we administer 1 g of intravenous cefazolin (or other broad-spectrum antibiotic) at the beginning of the procedure in order to minimize any risk of infection. Temperatures at the site of injection are typically well in excess of 50°C due to polymerization, helping to keep the injection site sterile.[13] The temperature increase may be an important factor in pain relief by cauterizing local nerve fibres.
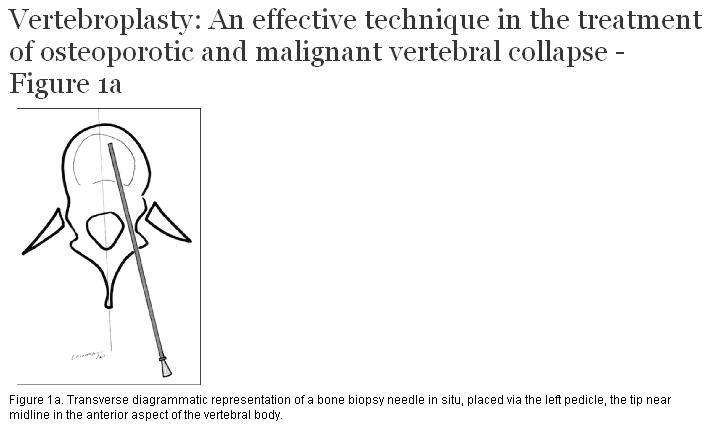
We have found that in most instances the best way to perform vertebroplasty is under fluoroscopic guidance using biplane fluoroscopy. High-quality imaging is critical for the successful and safe performance of this procedure, as poor imaging and lack of experience with embolization procedures are the principal factors blamed in most reports of major complications. Using fluoroscopic guidance, the radiologist guides an 11-gauge or 13-gauge bone biopsy needle down the barrel of the pedicle (Figure 1a, 1b). The tip of the needle is placed within the vertebral body near the midline, approximately at the junction of the anterior one-third with the posterior two-thirds of the vertebral body. A mixture of thick polymethylmethacrylate cement opacified with barium is then injected under continuous fluoroscopic guidance.[14] The addition of supplementary sterile barium is essential, as commercially available preparations are insufficiently radiodense to ensure adequate visibility during injection (Figure 2a-b, 2c, 2d, and 2e-j). Vigilant imaging is critical to avoid extravasation of cement, either into the venous system, foramina, or other undesirable extravertebral sites. In general, only a small quantity of cement—producing only partial filling of the vertebral body—is required to achieve satisfactory clinical results (2 mL to 7 mL).[15-17]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In many instances a single injection through one pedicle is all that is required.[14,18,19] If there is insufficient filling of the vertebral bodies, a second puncture through the contralateral pedicle is performed. Two or three levels can be treated at the same sitting if required. Treating more than three levels at a single sitting is seldom indicated. Risk of cardiovascular instability from by-products of the polymerizing injected cement is controversial. Although well described in the orthopedic literature, the small quantities used in vertebroplasty pose less of a risk.[20,21]
Pain relief from osteoporotic compression fractures with vertebroplasty is typically excellent, with more than 90% of patients describing complete or near complete relief of pain within 48 to 72 hours.[1,15,17,22-26] Further gradual improvement in pain has been reported to occur in the first 6 months.[23] Patients with metastatic disease show less dramatic improvement, with the rates on average being in the 70% range, although some series have reported figures much higher than this.[14,27]
In most centres, patients are now treated on an outpatient basis. Patients are treated early in the morning (the procedure taking approximately 1 hour), and are kept in the recovery area for approximately 4 to 6 hours. Patients with metastatic disease, who are often considerably more debilitated, may require overnight stays. We routinely perform follow-up CT scanning after injection of cement in order to assess cement distribution and ensure that there has been no inadvertent leakage in an undesirable location.
Local experience accrued until the time of writing consists of 11 patients, all of whom had lesions in the lower thoracic and lumbar region. In 10 cases compression fractures were secondary to underlying osteoporosis, and one patient had metastases from breast carcinoma. Of those with osteoporosis, 8 had near complete pain relief, and 2 partial improvement. The single patient with malignant disease had partial improvement that permitted significantly improved mobility. No complications were encountered.
Most large series demonstrate exceedingly few complications. The rate of complication varies considerably and depends substantially on the cause of the underlying lesion.[28] Complication rates are highest with patients who have metastatic disease and lowest in patients with osteoporotic compression fractures. Complications relate principally to leakage of cement, causing compression of adjacent structures or inadvertent injection into the vertebral venous plexus.[7,25] Either of these complications may produce compression of nerve roots or the spinal cord. Over-injection of the veins can also result in pulmonary embolism of cement.[29] Complications requiring surgery were reported in less than 3% of cases in a large series of over 250 patients (of which almost half were patients with metastatic disease).[1] Transient pain due to cement leakage—which resolves with conservative therapy—can be encountered in up to 10% of patients.
The most important factors to minimize complications include the following:[17,26]
• Appropriate radiographic equipment allowing precise placement of needle and monitoring of injected cement.
• Adequate opacification of cement.
• Operator training and experience.
In recent years it has become evident that excellent results can be achieved using minimal amounts of cement. This has the advantage of not making the vertebral body excessively stiff, thereby avoiding putting excessive stress on adjacent vertebral bodies, and also minimizing the possibility of inadvertent cement leakage. Some investigators with a series of more than 200 patients have not reported any symptomatic complication, or complications that have required any treatment.[14]
New cements are currently being developed for use in vertebroplasty. Some of these have augmented radio-opacity, allowing improved visualization. Others are “biocompatible,” containing hydroxyapatite. This cement may permit better incorporation and its diminished stiffness may decrease the risk of increased stress on adjacent vertebral bodies.[30]
Kyphoplasty has recently been introduced. In this procedure, a larger needle is inserted through a drill hole at the posterolateral aspect of the vertebral body, permitting placement of a balloon within the fractured segment. This is then filled with cement, reportedly restoring some lost vertebral body height.[31] This procedure is somewhat more expensive and technically more difficult, and its use remains controversial. A clinical trial directly comparing kyphoplasty and vertebroplasty may occur in the future.
With proper equipment and training, vertebroplasty appears to be an extremely safe and readily performed procedure. Symptomatic improvement can be expected and is usually dramatic. Issues that have not been addressed include direct comparison with surgical and conservative therapy, for which no randomized clinical trials exist. Because many third-party payers are now happy to pay for a procedure as inexpensive and safe as vertebroplasty, the running of such a trial will undoubtedly be challenging. Long-term outcomes are not yet fully known and will likely be slow to sort out, as many of these patients are elderly, with numerous co-morbid conditions.[32] What has become clear is that vertebroplasty will unquestionably play a key role in patients with vertebral compression fractures.
Availability of this technique in British Columbia is currently limited to a single centre. Numerous centres throughout the United States and Canada routinely offer this service. An excellent patient information resource and a partial listing of radiologists performing vertebroplasty is available on the web site of the Society of Interventional Radiology/Society of Cardiovascular and Interventional Radiology (www.scvir.org/patient/vertebro/index.htm).
We would like to thank several of our colleagues for their encouragement and aid with this project, including Drs Lindsay Machan, Mike Martin, Chris Morris, Doug Graeb, Gerald Legiehn, and Mr Lorie Marchinkow, RTR.
None declared.
References
1. Cotten A, Boutry N, Cortet B, et al. Percutaneous vertebroplasty: State of the art. Radiographics 1998;18:311-320. PubMed Abstract
2. Dean JR, Ison KT, Gishen P. The strengthening effect of percutaneous vertebroplasty. Clin Radiol 2000;55:471-476. PubMed Abstract
3. Deramond H, Depriester C, Galibert P, et al. Percutaneous vertebroplasty with polymethylmethacrylate: Technique, indications, and results. Radiol Clin North Am 1998;36:533-546. PubMed Abstract
4. Galibert P, Deramond H, Rosat P, et al. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie 1987;33:166-168. PubMed Abstract
5. Kaemmerlen P, Thiesse P, Bouvard H, et al. Percutaneous vertebroplasty in the treatment of metastases—Technique and results. J Radiol 1989;70:557-562. PubMed Abstract
6. Kaemmerlen P, Thiesse P, Jonas P. Percutaneous injection of orthopedic cement in metastatic vertebral lesions [letter]. N Engl J Med 1989;321:121. PubMed Citation
7. Murphy KJ, Lin DDM. Vertebroplasty: A simple solution to a difficult problem. J Clin Densitometry 2001;4:189-197. PubMed Citation
8. Mathis JM, Petri M, Naff N. Percutaneous vertebroplasty treatment of steroid-induced osteoporotic compression fractures. Arthritis Rheum 1998;41:171-175. PubMed Abstract
9. Tamayo-Orozco J, Arzac-Palumbo P, Peón-Vidales H, et al. Vertebral fractures associated with osteoporosis: Patient management. Am J Med 1997;103:44S-50S. PubMed Abstract
10. Peh WC, Gilula LA, Peck DD. Percutaneous vertebroplasty for severe osteoporotic vertebral body compression fractures. Radiology 2002;223:121-126. PubMed Abstract
11. Kaufmann TJ, Jensen ME, Schweickert PA, et al. Age of fracture and clinical outcomes of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2001;22:1860-1863. PubMed Abstract
12. O’Brien JP, Sims JT, Evans AJ. Vertebroplasty in patients with severe vertebral compression fractures: A technical report. AJNR Am J Neuroradiol 21:1555-1558. PubMed Abstract
13. Deramond H, Wright NT, Belkoff SM. Temperature elevation caused by bone cement polymerization during vertebroplasty. Bone 1999;25:17S-21S. PubMed Abstract
14. Lin DDM, Gailloud P, Murphy KJ. Percutaneous vertebroplasty in benign and malignant disease. Neurosurgery Quarterly 2002;11:290-301.
15. Cotten A, Dewatre F, Cortet B, et al. Percutaneous vertebroplasty for osteolytic metastases and myeloma: Effects of the percentage of lesion filling and the leakage of methyl methacrylate at clinical follow-up. Radiology 1996;200:525-530. PubMed Abstract
16. Belkoff SM, Mathis JM, Jasper LE, et al. The biomechanics of vertebroplasty—The effect of cement volume on mechanical behavior. Spine 2001;26:1537-1541. PubMed Abstract
17. Martin JB, Sugiu BJK, Ruíz DSM, et al. Vertebroplasty: Clinical experience and follow-up results. Bone 1999;25:11S-15S. PubMed Abstract
18. Tohmeh AG, Mathis JM, Fenton DC, et al. Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine 1999;24:1772-1776. PubMed Abstract
19. Kim AK, Jensen ME, Dion JE, et al. Unilateral transpedicular percutaneous vertebroplasty: Initial experience. Radiology 2002;222:737-741. PubMed Abstract
20. Kaufmann TJ, Jensen ME, Ford G, et al. Cardiovascular effects of polymethylmethacrylate use in percutaneous vertebroplasty. AJNR Am J Neuroradiol 2002;23:601-604. PubMed Abstract
21. Vasconcelos C, Gailloud P, Martin JB, et al. Transient arterial hypotension induced by polymethylmethacrylate injection during percutaneous vertebroplasty. J Vasc Interv Radiol 2001:12;1001-1002. PubMed Citation
22. Tsou IY, Goh PY, Peh WC, et al. Percutaneous vertebroplasty in the management of osteoporotic vertebral compression fractures: Initial experience. Ann Acad Med Singapore 2002;31:15-20. PubMed Abstract
23. Zoarski GH, Snow P, Olan WJ, et al. Percutaneous vertebroplasty for osteoporotic compression fractures: Quantitative prospective evaluation of long-term outcomes. J Vasc Interv Radiol 2002;13:139-148. PubMed Abstract
24. Cortet B, Cotten A, Boutry N. Percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fractures: An open prospective study. J Rheumatol 1999;26:2222-2228. PubMed Abstract
25. Cyteval C, Sarrabère MPB, Roux JO, et al. Acute osteoporotic vertebral collapse: Open study on percutaneous injection of acrylic surgical cement in 20 patients. AJR Am J Roentgenol 1999;173:1685-1690. PubMed Abstract
26. Barr J, Barr MS, Lemley TJ, et al. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine 2000;25;923-928. PubMed Abstract
27. Weill A, Chiras J, Simon JM, et al. Spinal metastases: Indications for and results of percutaneous injection of acrylic surgical cement. Radiology 1996;199:241-247. PubMed Abstract
28. Chiras J, Depriester C, Weill A, et al. Percutaneous vertebral surgery. Technics and indications. J Neuroradiol 1997;24:45-59. PubMed Abstract
29. Padovani B, Kasriel O, Brunner P, et al. Pulmonary embolism caused by acrylic cement: A rare complication of percutaneous vertebroplasty. AJNR Am J Neuroradiol 1999;20:375-377. PubMed Abstract
30. Belkoff MS, Mathis JM, Jasper LE, et al. An ex vivo biomechanical evaluation of a hydroxyapitite cement for use with vertebroplasty. Spine 2001;26:1542-1546. PubMed Abstract
31. Watts NB, Harris ST, Genant HK. Treatment of painful osteoporotic vertebral fractures with percutaneous vertebroplasty or kyphoplasty. Osteoporos Int 2001;12:429-437. PubMed Abstract Full Text
32. Grados F, Depriester C, Cayrolle G, et al. Long-term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology 2000;39:1410-1414. PubMed Abstract Full Text
P.L. Munk, MD, CM, FRCPC, and S.G.F. Ho, MD, FRCPC
Dr Munk is a radiologist at Vancouver Hospital and Health Sciences Centre, head of the Musculoskeletal Division, and a professor in the Department of Radiology at the University of British Columbia. Dr Ho is a radiologist at Vancouver Hospital and Health Sciences Centre, head of the Gastrointestinal Division, and assistant professor in the Department of Radiology at UBC.