The triple burden experienced by incarcerated people in British Columbia: Mental illness, substance use, and poverty
Issue: BCMJ,
vol. 68, No. 3, April 2026,
Pages 100-104 Original Research
ABSTRACT
Background: People transitioning from incarceration into the community often experience adverse health outcomes driven by the social determinants of health. This study aimed to compare the prevalence of mental health and substance use disorders and their associations with poverty and housing instability among people incarcerated in British Columbia provincial correctional centres versus the general community population.
Methods: We used linked administrative data on a random 20% sample of BC residents enrolled in public health insurance. Individuals with any provincial incarceration in 2015 or 2021 were identified and compared with nonincarcerated individuals in those years. Prevalence of mental illness, substance use disorders, and indicators of social disadvantage (income assistance, no fixed address) were calculated for both groups. In 2021, the sample included 1933 incarcerated people and 962 421 nonincarcerated people.
Results: Incarcerated people had significantly higher rates of mental illness and substance use disorder (including opioid and stimulant use disorders) than the community population. In 2021, 51.1% of incarcerated people had a diagnosed mental illness, 58.9% had a substance use disorder, and 41.0% had both. Co-occurring mental illness and substance use disorder were frequently associated with extreme poverty and housing instability. Nearly one-third (32.5%) of incarcerated people in 2021 had co-occurring mental illness and substance use disorder and either received income assistance or had no fixed address. Mental illness, substance use disorder, and poverty were much less common in the community cohort.
Conclusions: Incarcerated people in BC experience a triple burden of mental illness, substance use disorders, and socioeconomic marginalization (poverty and homelessness). There is an urgent need for targeted interventions during incarceration (e.g., evidence-based mental health and substance use disorder treatment) and greater postrelease support (housing, social services, and employment opportunities) to reduce health inequities and break the cycle of recidivism.
Comprehensive treatment for mental illness and substance use disorder is needed in provincial correctional centres, and postrelease supports must link people with housing, education, and employment opportunities.
Background
Health outcomes in Canada are shaped more by social determinants such as income and housing than by genetics or access to care.[1-3] Social determinants are especially influential for people who are experiencing mental illness and substance use disorders.[4-7] The COVID-19 pandemic intensified pressures on housing affordability, food insecurity, and homelessness across Canada.[8-10] In British Columbia, where housing costs are the highest in Canada, these pressures have evolved into a province-wide “cost of living crisis.”[9-12] These challenges are not experienced equally across the population.[13] People who are already experiencing social, economic, and health inequities are more likely to bear the burden of rising inequalities, which leads to outcomes such as premature mortality.[13]
Although the links between poverty, housing insecurity, and health are well established, little research has examined how these factors are associated with incarceration in Canada. Incarcerated people have distinct and often complex health profiles, but population-level evidence remains sparse.[4,5] In 2023–2024, 96.2% of admissions to Canadian correctional centres were to provincial or territorial facilities, which house people who are awaiting trial or serving sentences of less than 2 years.[14] In 2024, there were 9701 admissions to provincial correctional centres in BC.[15] People incarcerated in provincial correctional centres can quickly cycle between pretrial correctional centres, hospitals, and homelessness when released back into the community, which contributes to elevated rates of overdose mortality in the 2 weeks postrelease.[16] Unlike in the federal correctional system, there is no gradual return to community for people incarcerated in provincial correctional centres, and people can be released quickly from court without prescriptions or a warm handoff.[17] Understanding the associations between incarceration and social determinants of health is critical for designing health and social services that address the structural inequities experienced by incarcerated people that contribute to health outcomes, recidivism, and reintegration.
This study sought to measure the prevalence of mental illness, chronic diseases, and substance use disorder among incarcerated and nonincarcerated people in BC; assess changes in the prevalence of these conditions between 2015 and 2021; and describe how poverty and housing instability are associated with health conditions among incarcerated people.
Methods
Data source
Data were obtained from the BC Provincial Overdose Cohort (BC-ODC), a linked administrative database that includes a reference cohort that contains a 20% random sample of residents enrolled in BC’s public health insurance program. Each person was assigned a unique identifier to facilitate linkage across administrative data sets, including physician billing claims, hospitalizations, emergency department visits, pharmacy dispensations, provincial incarceration records, social assistance records, and death registrations. Longitudinal data were available from 1 January 2010 to 31 December 2021. Further details on the BC-ODC are available elsewhere.[18] People included in the BC-ODC were identified as incarcerated in 2021 if they had a BC Corrections admission that year. If they did not, they were assigned to the nonincarcerated group in 2021. This was repeated for 2015 to compare results from 2021 and 2015. This study was approved by the UBC Behavioural Research Ethics Board (#H23-02009).
Measures
For each individual in the sample, data from the previous 5 years were used to determine substance use conditions, withdrawal syndrome, and social determinants of health (income assistance and no fixed address). Chronic physical health conditions (circulatory disease, diabetes, inflammatory disease, kidney disease, neurological disease, and respiratory disease) were determined using all available years of data beginning from 1 January 2010. The reference time frame ended on 31 December of the record year (2015 or 2021) for people who were not incarcerated and the day before admission to a correctional centre for people who were incarcerated. Definitions of terms used throughout the article are provided in a Supplementary Information file.
Statistical analysis
Descriptive statistics were used to calculate the prevalence of health conditions and social determinants of health in the two groups (incarcerated and nonincarcerated) and for the 2 years under study (2015 and 2021). A two-sample binomial test of proportions with a two-sided alternative hypothesis was used to identify a statistically significant difference in the prevalence of a health condition between incarcerated and nonincarcerated groups. Because we aimed to describe the health status of the overall population of correctional centres and the community, we did not match or adjust for age or sex differences between the populations.
Results
 The sample in 2015 included 3306 people who were incarcerated that year and 917 174 people who were not incarcerated. The 2021 sample included 1933 people who were incarcerated that year and 962 421 people who were not incarcerated. People who were incarcerated in 2021 were primarily male (n = 1753, 91%), and the median age was 35 years (IQR: 29, 43). In contrast, the nonincarcerated (community) group was 49% male (n = 475 368) and had a median age of 47 years (IQR: 32, 63).
The sample in 2015 included 3306 people who were incarcerated that year and 917 174 people who were not incarcerated. The 2021 sample included 1933 people who were incarcerated that year and 962 421 people who were not incarcerated. People who were incarcerated in 2021 were primarily male (n = 1753, 91%), and the median age was 35 years (IQR: 29, 43). In contrast, the nonincarcerated (community) group was 49% male (n = 475 368) and had a median age of 47 years (IQR: 32, 63).
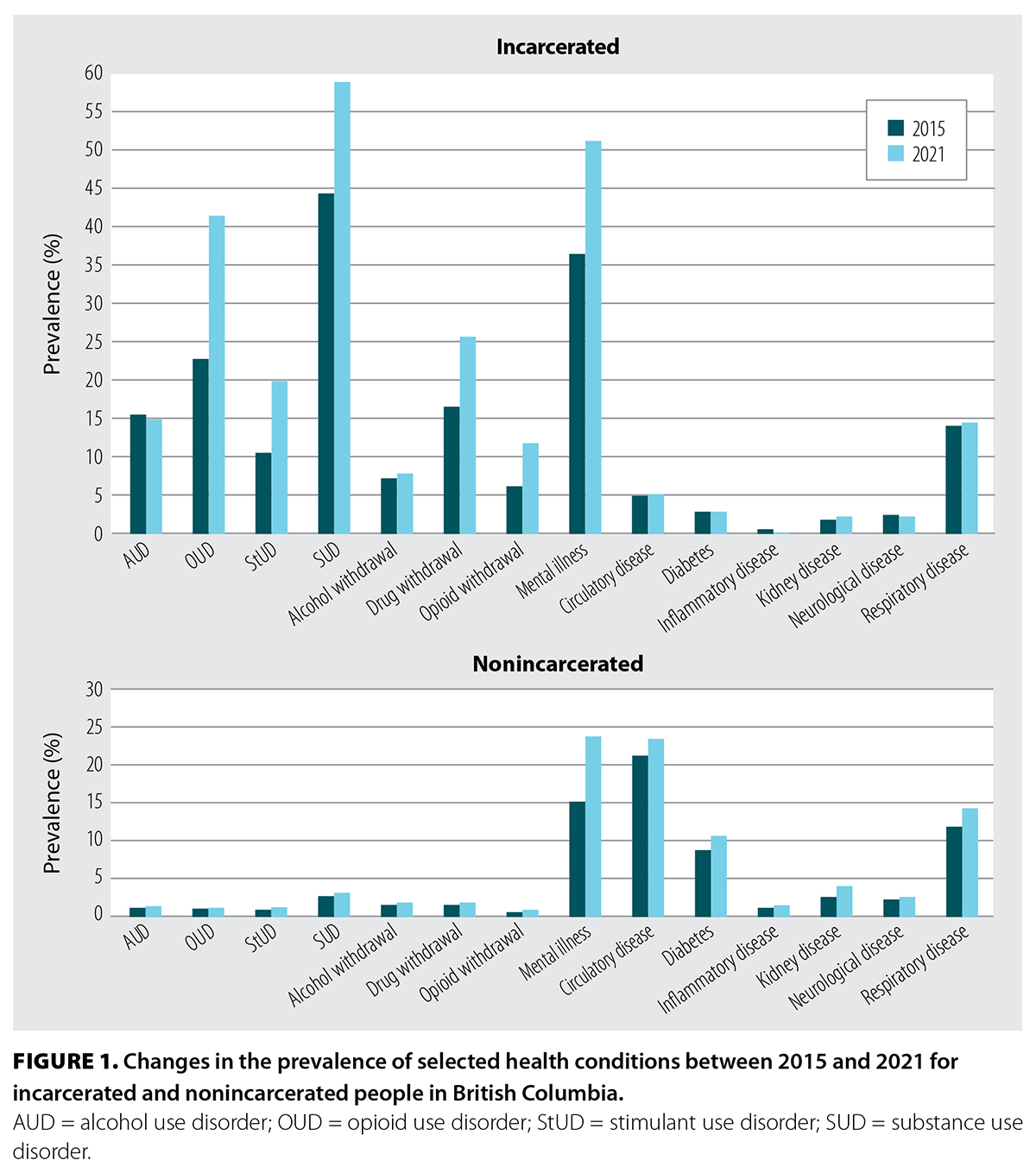
In 2021, all substance use disorders were more prevalent among incarcerated people than those who were not incarcerated. Substance use disorder occurred among 58.9% of incarcerated people versus 3.2% of nonincarcerated people (P < .001). Opioid use disorder occurred in 41.4% of incarcerated people compared with 1.2% of nonincarcerated people (P < .001). The prevalence of chronic physical conditions was either similar between incarcerated and nonincarcerated people or higher among the nonincarcerated group, which could be attributed to population demographic characteristics. From 2015 to 2021, opioid use disorder, stimulant use disorder, substance use disorder, substance withdrawal, and mental illness all became more prevalent among incarcerated people [Figure 1].
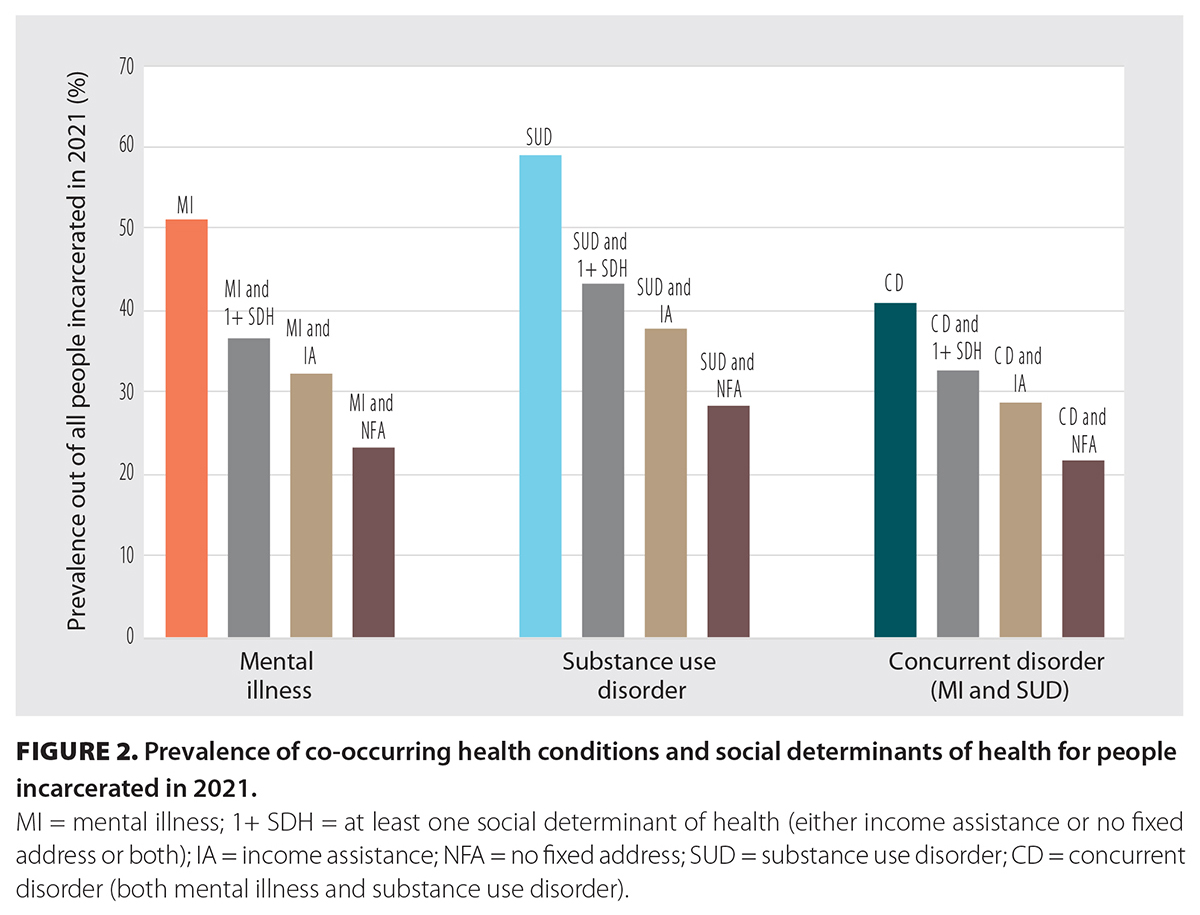 Mental illness and substance use disorder commonly co-occurred among those with no fixed address who were receiving social assistance. In 2021, 51.1% of incarcerated people had been previously diagnosed with a mental illness, while 36.7% had a mental illness and no fixed address and/or were receiving social assistance [Figure 2]. Similarly, 58.9% of incarcerated people had substance use disorder, and 43.4% had both substance use disorder and a record of no fixed address and/or social assistance. In 2021, mental illness and substance use disorder co-occurred among 41.0% of incarcerated people, and 32.5% had co-occurring mental illness, substance use disorder, and no fixed address and/or social assistance.
Mental illness and substance use disorder commonly co-occurred among those with no fixed address who were receiving social assistance. In 2021, 51.1% of incarcerated people had been previously diagnosed with a mental illness, while 36.7% had a mental illness and no fixed address and/or were receiving social assistance [Figure 2]. Similarly, 58.9% of incarcerated people had substance use disorder, and 43.4% had both substance use disorder and a record of no fixed address and/or social assistance. In 2021, mental illness and substance use disorder co-occurred among 41.0% of incarcerated people, and 32.5% had co-occurring mental illness, substance use disorder, and no fixed address and/or social assistance.
Discussion
This study shows that in BC, incarcerated people face a disproportionate burden of mental illness, substance use disorders, and socioeconomic disadvantage compared with people who are not incarcerated. Incarcerated people were younger than nonincarcerated people, and although they had fewer chronic physical conditions, they had a far higher prevalence of mental illness and substance use disorder. These conditions were frequently associated with income assistance and housing instability, which created a triple burden of health and social inequities.
Additionally, the prevalence of mental illness and substance use disorder among incarcerated people increased between 2015 and 2021. Rates of mental illness and co-occurring substance use disorder are increasing in BC’s provincial correctional system, often in combination with homelessness and poverty postrelease. Prior research has described “social sedimentation,” where health inequities concentrate among low-income groups and reproduce across generations.[13] Poverty and housing insecurity are linked to recidivism risk.[19] People in BC who have concurrent disorders have among the highest reincarceration rates: 72% return to custody within 3 years.[20] Correctional facilities provide a key point of intervention to reverse cycles of disadvantage. Robust prerelease discharge planning is urgently needed in provincial institutions to ensure people leaving custody have access to stable housing, health care, income supports, employment, and education services.
Study limitations
Our study had several limitations. We conducted a descriptive, population-based study using linked administrative data. We did not adjust for demographic differences between the incarcerated and nonincarcerated groups, because our goal was to describe entire populations rather than estimate adjusted effects. Our estimates reflect 2015 and 2021 trends among a random sample of people enrolled in public health insurance in BC. Custody volumes and health care delivery inside and outside of correctional centres changed during the COVID-19 pandemic.[21] Since 2021, the toxic drug crisis has also intensified, and the association between substance use disorder, homelessness, and postrelease overdose risk could be underrepresentative of the postpandemic period.[16]
Conclusions
Incarceration is a critical time to disrupt entrenched cycles of poverty. Resources are needed to implement comprehensive mental illness and substance use disorder treatment in provincial correctional centres and the community. Postrelease supports must be strengthened, with a focus on linking people with housing, education, and employment opportunities alongside expanded access to community-based mental health and substance use disorder treatment.
Acknowledgments
This study was funded by the Canadian Institutes of Health Research and Michael Smith Health Research BC. We acknowledge, with gratitude, the traditional, unceded, and ancestral territories of the Musqueam Nation, Squamish Nation, Tsleil-Waututh Nation, and Kwikwetlem First Nation in Vancouver, where BC Mental Health and Substance Use Services, the BC Centre for Disease Control, and the University of British Columbia are based. We also recognize the important contributions of Priorities and Engagement in Research in Correctional Health, British Columbia to this project and the work of the Canadian Collaboration for Prison Health and Education. Access to data provided by the data stewards is subject to approval but can be requested for research projects through the data stewards or their designated service providers. The following data sets were used in this study: Medical Services Plan, PharmaNet, Discharge Abstract Database, National Ambulatory Care Reporting System, incarceration records data from the BC Ministry of Public Safety and Solicitor General, social assistance data from the BC Ministry of Social Development and Poverty Reduction, the Chronic Disease Registry, BC Vital Statistics Agency records, and BC Coroners Service records. All inferences, opinions, and conclusions drawn in this article are those of the authors and do not reflect the opinions or policies of the data stewards. These data were provisioned under Information Sharing Agreement J16-145.
Competing interests
A.S. received project funding from Michael Smith Health Research BC for the submitted work and project grant funding from the Canadian Institutes for Health Research, BC Ministry of Health, Public Health Agency of Canada, and Health Canada. A.M. received honoraria and speaker’s fees from Indivior and the Master Clinician Alliance. A.M. is a member of the Indivior national advisory board. A.K. received speaker and advisory committee honoraria from Lundbeck, Eisai, Idorsia, and Otsuka. The remaining authors have no competing interests to declare.
- Supplementary information
-
Case definitions
Income assistance: At least one monthly record in the BC Ministry of Social Development and Poverty Reduction (SDPR) data set indicating that income assistance was received, OR a dispensation record in PharmaNet with plan type = C. If either of these conditions was met in the 5 years prior to 31 December of year X, then the person was considered to meet the conditions for income assistance in year X.
No fixed address: At least three consecutive monthly records in the SDPR data set indicating no fixed address, OR at least one record in the Medical Services Plan (MSP) data set with ICD code of V60.0 or V60.1, OR at least one record in the Discharge Abstract Database (DAD) data set with a code of Z59.0 or Z59.1. If any of these conditions were met in the 5 years prior to 31 December of year X, then the person was considered to meet the conditions for no fixed address in year X.
Mental illness: For each of anxiety, depression, schizophrenia, bipolar disorder, and stress disorder, at least two MSP records containing the relevant ICD-9 codes (below) within the same 12-month period, OR one DAD record with the relevant ICD-10 code (below). If the requirements for any of anxiety, depression, schizophrenia, bipolar disorder, or stress disorder were met at any time prior to 31 December of year X, then the requirements for mental illness were met in year X.
Anxiety: ICD-9 codes 300, excluding 300.4 and 50B; ICD-10 codes F40, F41.
Depression: ICD-9 codes 300.4, 311, 50B; ICD-10 codes F31, F33, F34.1.
Schizophrenia: ICD-9 codes 295, 297, 298; ICD-10 codes F20, F21, F22, F23, F24, F25, F28, F29.
Bipolar disorder: ICD-9 codes 296; ICD-10 codes F30, F31, F34, F38, F39, excluding F34.1.
Stress disorder: ICD-9 codes 308, 309; ICD-10 codes F43.
Substance use disorder: At least two MSP records in the same 12-month period with code 291, 292, 303, 304, or 305 and not 3051, OR one DAD record with code F10, F11, F12, F13, F14, F15, F16, F17, F18, or F19, OR the conditions for opioid use disorder are met. If any of these conditions were met in the 5 years prior to 31 December of year X, then the person was considered to have substance use disorder in year X.
Opioid use disorder: At least two MSP records in the same 12-month period with code 3040, 3047, or 3055, OR one DAD record with code F11, OR one PharmaNet record with code 999792, 999793, 66999990, 66999991, 66999992, 6999993, 66999997, 66999998, 6999999, 67000000, 67000001, 67000002, 67000003, 67000004, 67000005, 67000006, 67000007, 67000008, 67000009, 67000010, 67000011, 67000012, 67000013, 67000014, 67000015, 67000016, 67000017, 67000018, 67000019, 67000020, 2295695, 2295709, 2408090, 2408104, 2424851, 2424878, 2453908, 2453916, 2468085, 2468093, 2502313, 2502321, 2502348, 2502356, 2517175, 2517183, 22123346, 22123347, 2123348, 22123349, 2019930, 2019949, 2019957, 2019965, 2177749, or 2177757. If any of these conditions were met in the 5 years prior to 31 December of year X, then the person was considered to have opioid use disorder in year X.
Stimulant use disorder: At least two MSP records in the same 12-month period with code 3042, 3052, 3044, or 3057, OR one DAD record with code F14 or F15. If either of these conditions was met in the 5 years prior to 31 December of year X, then the person was considered to have stimulant use disorder in year X.
Alcohol use disorder: At least two MSP records in the same 12-month period with code 291, 303, or 3050, OR one DAD record with code F10. If either of these conditions was met in the 5 years prior to 31 December of year X, then the person was considered to have alcohol use disorder in year X.
Alcohol withdrawal: At least one MSP record with code 2910 or 29181, OR one DAD record with code F101, F102, or F109. If either of these conditions was met in the 5 years prior to 31 December of year X, then the person met the conditions for alcohol withdrawal in year X.
Opioid withdrawal: At least one DAD record with code F111, F112, or F119. If this condition was met in the 5 years prior to 31 December of year X, then the person met the conditions for opioid withdrawal in year X.
Drug withdrawal: At least one MSP record with code 2920, OR one DAD record with code F111, F112, F119, F131, F132, F139, F141, F142, F149, F151, F152, F159, F191, F192, or F199. If either of these conditions was met in the 5 years prior to 31 December of year X, then the person met the conditions for drug withdrawal in year X.
Circulatory disease: The Chronic Disease Registry (CDR) indicates acute myocardial infarction, OR angina, OR heart failure, OR hypertension, OR stroke (hospitalized case definition), OR stroke (hospitalized hemorrhagic case definition), OR stroke (hospitalized transient ischemic attack case definition), OR stroke (hospitalized ischemic case definition). If any of these conditions were met any time prior to 31 December of year X, then the person was considered to have circulatory disease in year X.
Diabetes: The CDR indicates diabetes. If this condition was met at any time prior to 31 December of year X, then the person was considered to have diabetes in year X.
Inflammatory disease: The CDR indicates rheumatoid arthritis. If this condition was met at any time prior to 31 December of year X, then the person was considered to have inflammatory disease in year X.
Kidney disease: The CDR indicates chronic kidney disease. If this condition was met at any time prior to 31 December of year X, then the person was considered to have kidney disease in year X.
Neurological disease: The CDR indicates Alzheimer disease/dementia, OR epilepsy, OR multiple sclerosis, OR Parkinson disease/Parkinsonism. If any of these conditions were met at any time prior to 31 December of year X, then the person was considered to have neurological disease in year X.
Respiratory disease: The CDR indicates asthma, OR chronic obstructive pulmonary disease. If either of these conditions was met at any time prior to 31 December of year X, then the person was considered to have respiratory disease in year X.
Chronic condition: If the person met the conditions for having any of circulatory disease, diabetes, inflammatory disease, kidney disease, neurological disease, or respiratory disease, then they were considered to have a chronic condition.
This article has been peer reviewed.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
References
1. Standing Senate Committee on Social Affairs, Science and Technology. A healthy, productive Canada: A determinant of health approach. The Standing Senate Committee on Social Affairs, Science and Technology Final Report of Senate Subcommittee on Population Health. 2009. Accessed 27 February 2025. https://sencanada.ca/content/sen/committee/402/popu/rep/rephealth1jun09-e.pdf.
2. Frank J, Abel T, Campostrini S, et al. The social determinants of health: Time to re-think? Int J Environ Res Public Health 2020;17:5856. https://doi.org/10.3390/ijerph17165856.
3. Donkin A, Goldblatt P, Allen J, et al. Global action on the social determinants of health. BMJ Glob Health 2017;3(Suppl 1):e000603. https://doi.org/10.1136/bmjgh-2017-000603.
4. Stewart LA, Nolan A, Thompson J, Power J. Social determinants of health among Canadian inmates. Int J Prison Health 2018;14:4-15. https://doi.org/10.1108/IJPH-08-2016-0038.
5. Kouyoumdjian F, Schuler A, Matheson FI, Hwang SW. Health status of prisoners in Canada: Narrative review. Can Fam Physician 2016;62:215-222.
6. Rotter M, Compton M. Criminal legal involvement: A cause and consequence of social determinants of health. Psychiatr Serv 2022;73:108-111. https://doi.org/10.1176/appi.ps.202000741.
7. Edwards LM, Chang S, Zeki R, et al. The associations between social determinants of health, mental health, substance-use and recidivism: A ten-year retrospective cohort analysis of women who completed the connections programme in Australia. Harm Reduct J 2024;21:2. https://doi.org/10.1186/s12954-023-00909-4.
8. Housing, Infrastructure and Communities Canada. Everyone counts 2020-2022: Preliminary highlights report. Modified 28 April 2023. Accessed 21 June 2025. https://housing-infrastructure.canada.ca/homelessness-sans-abri/reports-rapports/pit-counts-dp-2020-2022-highlights-eng.html.
9. Little S, Mosconi C. Surging cost of living leading to ‘inflation isolation’ in B.C.: Poll. Global News. 27 November 2023. Accessed 6 October 2024. https://globalnews.ca/news/10117901/cost-of-living-mental-health-isolation-b-c/.
10. Aerts A. The high cost of living in British Columbia. CPABC in Focus 2022;July/August:14-24. Accessed 5 October 2024. www.bccpa.ca/news-events/cpabc-newsroom/2022/july/the-high-cost-of-living-in-british-columbia/.
11. CBC News. Stress, isolation, feelings of failure: Rising costs are taking a toll on mental health this holiday season. CBC News. 19 December 2023. Accessed 6 October 2024. www.cbc.ca/news/canada/british-columbia/cost-of-living-impacts-b-c-1.7060037.
12. Williams D. Sticker shock: The rising price of everything in B.C. Business Council of British Columbia, 2024. Accessed 5 October 2024. www.bcbc.com/insight/sticker-shock-the-rising-price-of-everything-in-bc.
13. Ross MW. The need for correctional public health and health promotion. Health and health promotion in prisons. London, UK: Routledge; 2012. pp. 13-21. https://doi.org/10.4324/9780203083239.
14. Statistics Canada. Correctional services statistics: Interactive dashboard. Modified 4 March 2025. Accessed 24 October 2025. www150.statcan.gc.ca/n1/pub/71-607-x/71-607-x2019018-eng.htm.
15. British Columbia Ministry of Public Safety and Solicitor General. Adult custody statistics dashboard. Accessed 26 August 2024. https://app.powerbi.com/view?r=eyJrIjoiNzE2ZmM5MTMtN2U5ZC00ZGQ1LTk4YWUtY2UwNDdiYWI5NTQyIiwidCI6IjZmZGI1MjAwLTNkMGQtNGE4YS1iMDM2LWQzNjg1ZTM1OWFkYyJ9&pageName=ReportSection69506dda63e5b4460c64.
16. Kinner SA, Gan W, Slaunwhite A. Fatal overdoses after release from prison in British Columbia: A retrospective data linkage study. CMAJ Open 2021;9:E907-E914. https://doi.org/10.9778/cmajo.20200243.
17. Husein S, Taylor C. From incarceration to encampment: Why so many Ontario prisoners end up homeless. John Howard Society of Ontario, 2025. Accessed 24 October 2025. https://johnhoward.on.ca/wp-content/uploads/2025/07/Rethinking-Justice-Housing-Report-From-Incarceration-to-Encampment.pdf.
18. MacDougall L, Smolina K, Otterstatter M, et al. Development and characteristics of the Provincial Overdose Cohort in British Columbia, Canada. PLoS One 2019;14:e0210129. https://doi.org/10.1371/journal.pone.0210129.
19. Mitchell RJ, Burns N, Glozier N, Nielssen O. Homelessness and predictors of criminal reoffending: A retrospective cohort study. Crim Behav Ment Health 2023;33:261-275. https://doi.org/10.1002/cbm.2298.
20. Butler A, Nicholls TL, Samji H, et al. Mental health needs, substance use, and reincarceration: Population-level findings from a released prison cohort. Crim Justice Behav 2024;51:1054-1071. https://doi.org/10.1177/00938548241238327.
21. McLeod KE, Timler K, Korchinski M, et al. Supporting people leaving prisons during COVID-19: Perspectives from peer health mentors. Int J Prison Health 2021;17:206-216. https://doi.org/10.1108/IJPH-09-2020-0069.
Dr Slaunwhite is an assistant professor at the School of Population and Public Health, University of British Columbia; a director at the Canadian Collaboration for Prison Health and Education; and a scientific director at BC Mental Health and Substance Use Services. Ms Rondeau is a PhD student at the Canadian Collaboration for Prison Health and Education. Ms Roth is a project manager at the Canadian Collaboration for Prison Health and Education. Ms Budau is a research advisor at the Canadian Collaboration for Prison Health and Education and a coordinator on the Priorities and Engagement in Research in Correctional Health, British Columbia (PERCH BC) Advisory Committee, UBC. Mr Sabadash is a peer support worker at BC Mental Health and Substance Use Services and an advisor on the PERCH BC Advisory Committee, UBC. Dr Nicholls is a scientific director at BC Mental Health and Substance Use Services and a professor in the Department of Psychiatry, UBC. Dr Krishnamoorthy is a medical director at BC Mental Health and Substance Use Services and a clinical associate professor in the Department of Psychiatry, UBC. Dr Butler is an assistant professor in the School of Criminology, Simon Fraser University. Dr Mead is a medical director at BC Mental Health and Substance Use Services. Ms McQuarrie is a statistician at the Canadian Collaboration for Prison Health and Education.
Corresponding author: Amanda K. Slaunwhite, Amanda.Slaunwhite@ubc.ca.
