Clinical Case Reports
Third-degree heart block secondary to Lyme carditis
Issue: BCMJ,
vol. 65 , No. 10 , December 2023 ,
Pages 382-384 Clinical Articles Clinical Case Reports
ABSTRACT: Third-degree heart block is an uncommon but severe and potentially fatal complication of Lyme disease. We present the case of a previously healthy 42-year-old male with no prior cardiac history who developed persistent third-degree heart block and Bell palsy secondary to untreated Lyme disease. The patient later achieved complete symptomatic resolution with antibiotic therapy and avoided intervention via cardiac pacing. This case highlights a need for increased awareness of the clinical manifestations of Lyme disease and disseminated Lyme disease to improve patient outcomes and reduce potential complications.
Increased awareness of Lyme carditis is essential for prompt diagnosis; early antibiotic initiation; and prevention of pacing, complications, and death.
Case data
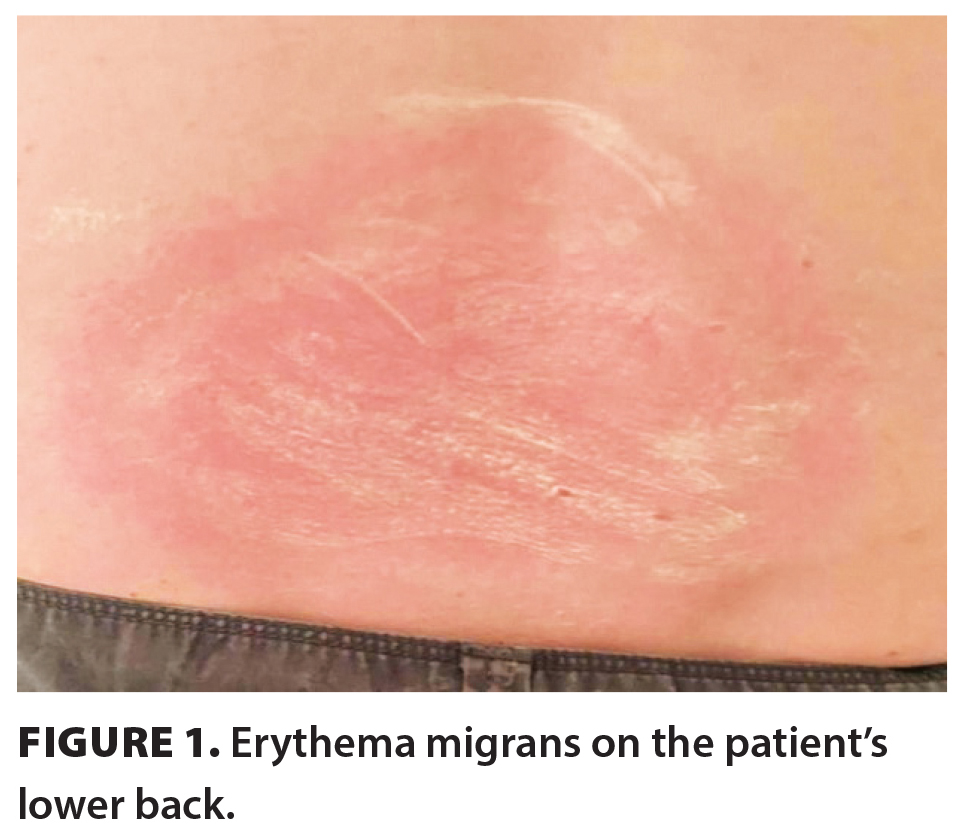
A previously healthy 42-year-old male with no cardiac history was admitted to hospital after presenting to the emergency department with presyncope and palpitations. Approximately 2 months prior, he had traveled extensively in Texas; northern Mexico; southeastern Ontario; and British Columbia. While in Ontario, he had resided in a cabin and received an insect bite. One week later, he developed erythema migrans [Figure 1], followed by fatigue. He presented to a walk-in clinic and was prescribed a 7-day course of cephalexin three times daily for a presumed spider bite. One week later, his skin manifestations spread to his neck and axillae, and he was provided a second 7-day course of cephalexin at a walk-in clinic.
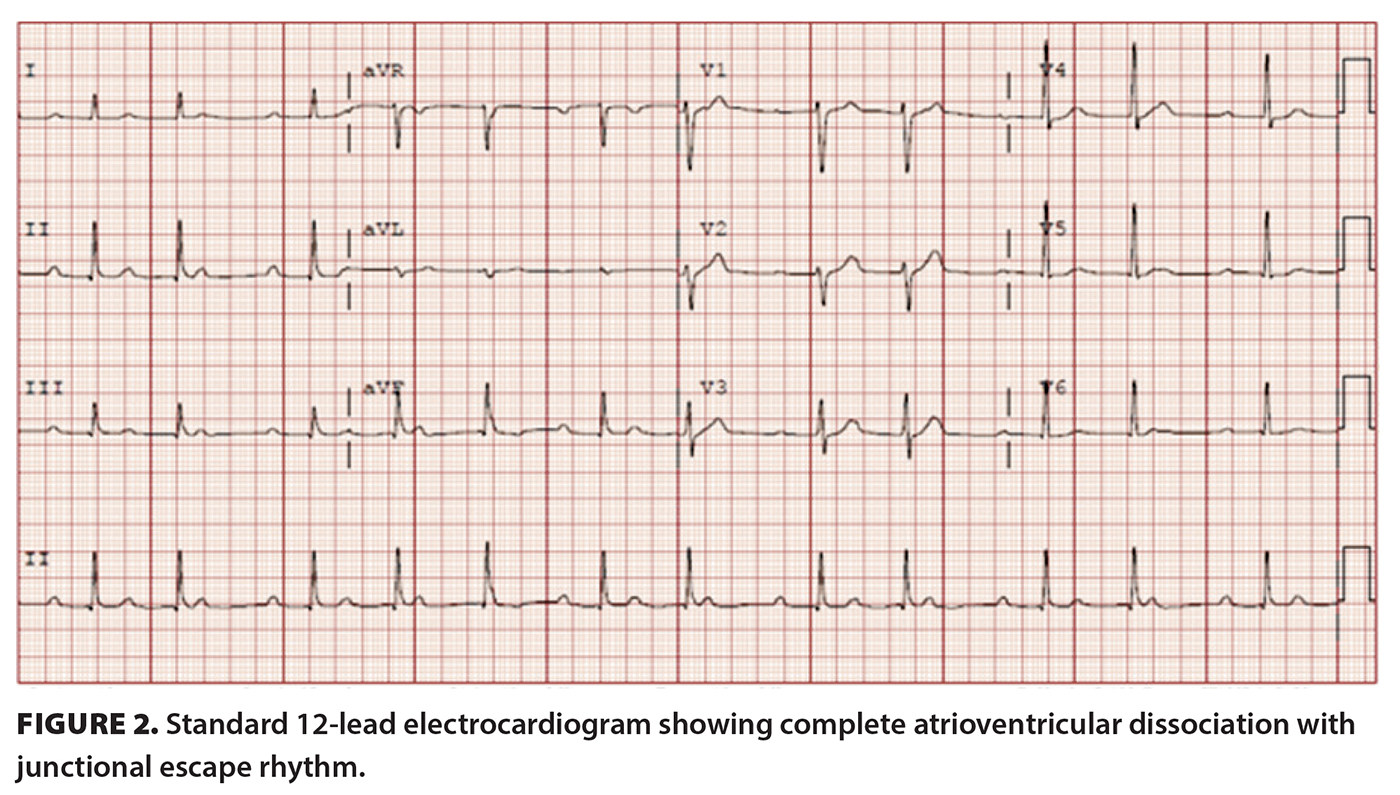
After developing heart palpitations and presyncope, the patient presented to the emergency department. Laboratory investigations, a chest X-ray, and an electrocardiogram (ECG) showed no abnormalities. However, 2 days later, he returned with a right eye droop, tongue numbness, and right lower lip numbness. He was diagnosed with Bell palsy and prescribed a course of prednisone and retroviral therapy, and Lyme serology was ordered. Approximately 10 days later, he returned with significant fatigue and heart palpitations. ECG revealed a complete atrioventricular dissociation with junctional escape rhythm [Figure 2]. Lyme serology returned positive and identified the presence of Borrelia burgdorferi. The remaining laboratory investigations were largely unremarkable.
The patient was started on IV ceftriaxone and was admitted to the cardiac unit, where he continued to suffer from heart palpitations and presyncope. Upon examination, he remained bradyarrhythmic, with a heart rate of 41 beats per minute, and had a slight right-sided facial droop. Telemetry revealed an intermittent atrioventricular block, and ECG showed sinus rhythm, premature atrial complexes, and a prolonged PR interval of 338 m/s. Repeat ECG showed sinus rhythm with a 2:1 heart block. A transthoracic echocardiogram revealed a third-degree atrioventricular block, with mild mitral regurgitation due to atrioventricular dissociation.
Five days after admission, the patient remained bradycardic with intermittent palpitations, and a complete third-degree atrioventricular block with a heart rate of 38 beats per minute was found on ECG and again upon repeat. A 2:1 atrioventricular block occurred the next day, which persisted. A cardiac MRI showed no abnormalities or evidence of myocardial edema, inflammation, scar, or infiltrative process. Ten days after admission, the patient returned to sinus bradycardia with second-degree type 1 atrioventricular block conduction. Repeat ECG showed sinus bradycardia with second-degree type 1 atrioventricular block. Clinically, the patient continued to improve with IV antibiotics.
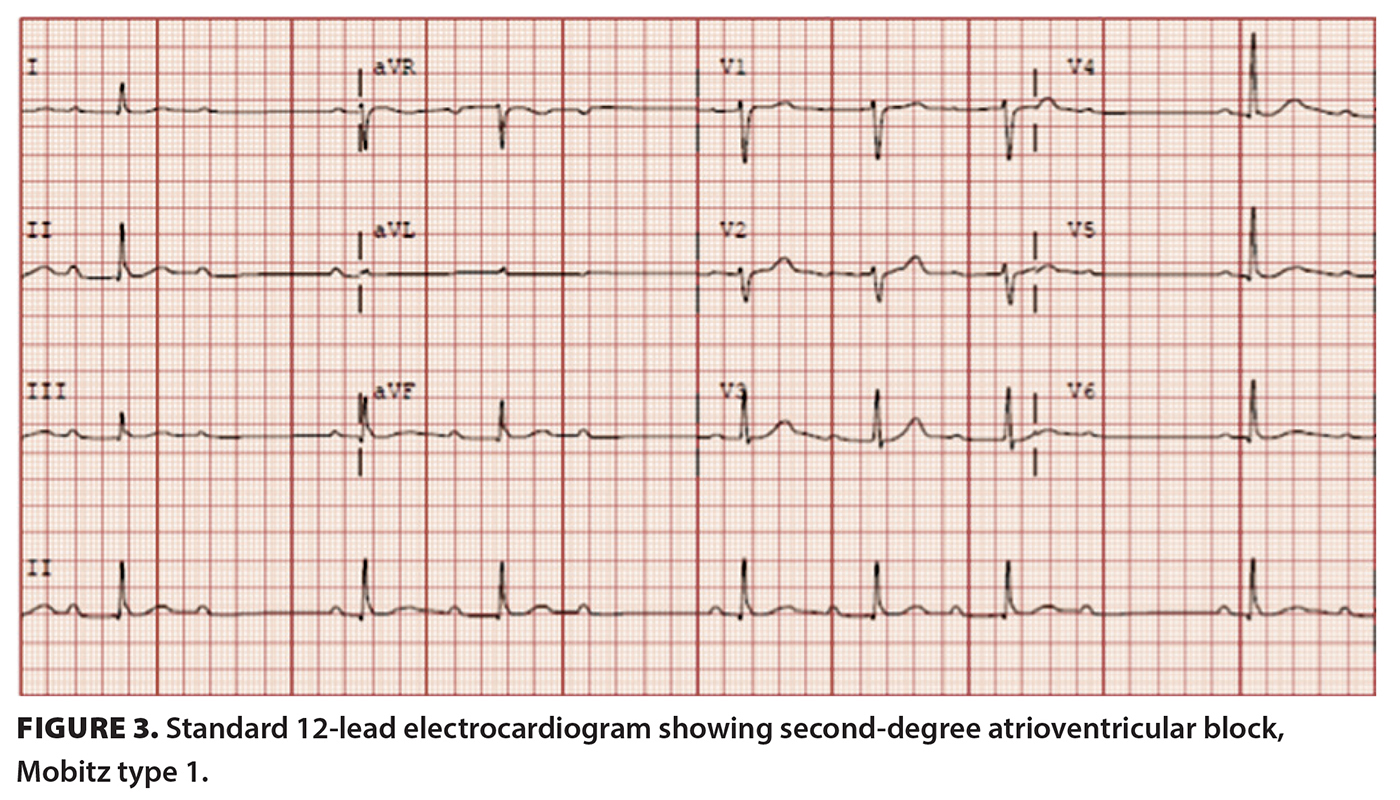
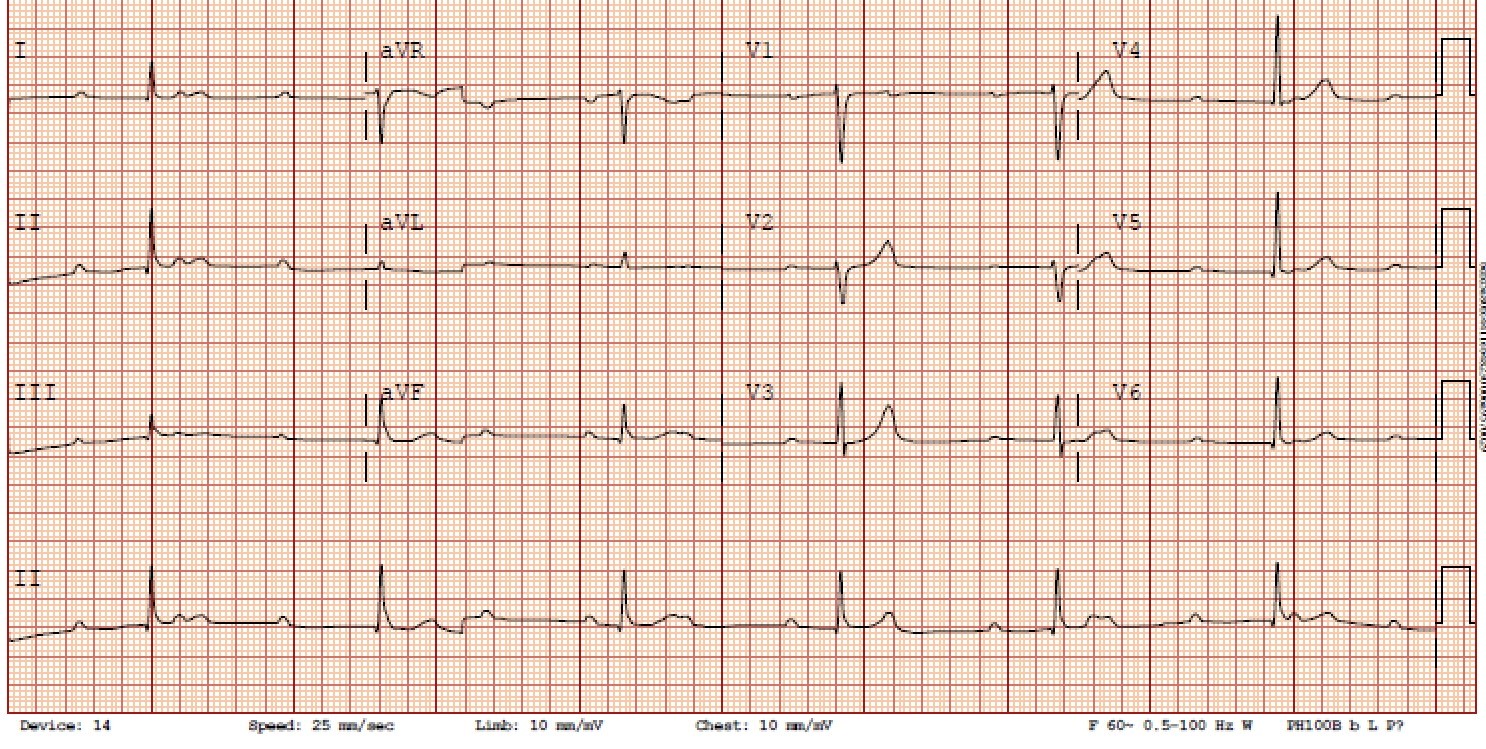
Upon discharge, ECGs demonstrated sinus rhythm with heart rates upward of 90 beats per minute, with intermittent first-degree atrioventricular block and intermittent second-degree type 1 atrioventricular block without evidence of higher-grade heart blocks [Figure 3].
With this improvement, the patient avoided intervention with temporary pacing. He was discharged on oral doxycycline 100 mg twice daily and was instructed to complete a 24-hour Holter monitor, with close follow-up with Kelowna General Hospital’s cardiology and infectious diseases services. An outpatient Holter monitor 19 days postdischarge depicted complete normalization of the conduction system without evidence of heart block or concerning arrhythmias. Nearly 3 months after the tick bite, the patient remained clinically at his baseline without any persisting symptoms.
Discussion
Epidemiology
Lyme disease, the tick-borne illness caused by the spirochete B. burgdorferi, has been recorded across North America. There is a known geographic expansion of the black-legged tick responsible for Lyme disease, Ixodes scapularis, which is thought to be associated with increasing global temperatures due to climate change.[1] As a result, increasing cases of Lyme disease have been reported throughout Canada, with most occurring in Ontario.[1]
Second- or third-degree heart block occurs in approximately 1% of reported Lyme disease cases.[2] The literature also reports a predominance of Lyme carditis occurring in teenaged to middle-aged males, with most cases occurring during the summer to late autumn.[3,4] While Lyme disease has a bimodal age distribution, third-degree atrioventricular block secondary to Lyme carditis predominantly affects those aged 10 to 45 years.[5] The case of the patient discussed in this study is consistent with others reported in the literature, including in terms of demographics, location, and time frame, which highlights that Lyme disease is an important consideration in young patients who present with atrioventricular block without an apparent cause.[3]
Clinical manifestation
Early Lyme disease typically presents with erythema migrans, fatigue, fever, myalgias, and arthralgias.[6] If left untreated, Lyme disease can disseminate over weeks to months, which can affect the central and peripheral nervous systems, joints, skin, and cardiovascular system.[6] However, with early recognition and antibiotic therapy, most patients do not progress to multisystem manifestations, such as Lyme carditis.[7]
All structures of the heart can be affected by the Lyme bacterium, including the myocardium, pericardium, endocardium, vasculature, valves, and atrioventricular node.[8] Lyme carditis develops when host immune cells detect the invading bacteria and results in inflammation and cardiac tissue damage, which can impair the electrical conduction system.[9] Most Lyme carditis cases lead to atrioventricular block, a cardiac manifestation that can be fatal.[9] The most common symptoms of Lyme carditis include shortness of breath, light-headedness, syncope, palpitations, and chest pain.[9]
Cardiac involvement of Lyme disease can present with varying severities of atrioventricular block, prolonged QT intervals, sinus node disease, and interventricular delay.[3] Atrioventricular block in Lyme carditis can fluctuate between first-, second-, and third-degree block, as occurred in our patient.[3] Transient, atrioventricular block can progress rapidly, with approximately one-third of patients requiring temporary pacing.[4] In our patient, the progression to third-degree atrioventricular block was rapid, occurring only weeks after the tick bite.
Treatment
The recommended duration of either oral or parenteral antibiotic therapy for patients with atrioventricular block and/or myopericarditis associated with early Lyme disease is 14 to 21 days.[10] Due to the fluctuating and rapidly progressive nature of Lyme carditis, it is recommended that symptomatic patients, those with second- or third-degree atrioventricular block, and those with first-degree atrioventricular block with a PR interval of 300 m/s or higher be hospitalized and provided with continuous monitoring and assessment by a cardiologist.[10] IV ceftriaxone 2 g daily is the recommended first-line antibiotic treatment for hospitalized or unstable patients; doxycycline 100 mg by mouth twice daily is recommended for outpatients.[10] If untreated, this rare but serious cardiac manifestation can be fatal. However, with appropriate antibiotic therapy, atrioventricular block can be reversed, and the overall prognosis can be excellent.[10] If symptoms remain refractory to medical management or if the patient is dangerously unstable, the standard treatment for high-degree atrioventricular block is transvenous or transcutaneous pacing. Rarely, a permanent pacemaker implantation is required.[7] Other complications of atrioventricular block induced by Lyme carditis include pericarditis, myocarditis, and death.[7]
Summary
Lyme carditis is a rare but severe manifestation of Lyme disease that can rapidly progress to third-degree atrioventricular block and death. Recognition and increased awareness of Lyme disease and Lyme carditis are essential for prompt diagnosis; early antibiotic initiation; and prevention of pacing, complications, and death. Furthermore, a detailed history of travel and outdoor activities is warranted in young, previously healthy patients who present with atrioventricular block. This case highlights the need for early identification of erythema migrans and an increased awareness of and clinical suspicion for Lyme disease and Lyme carditis.
Competing interests
None declared.
Acknowledgments
The authors thank the patient for his input, efforts to increase awareness of Lyme carditis, and willingness to participate in this project.
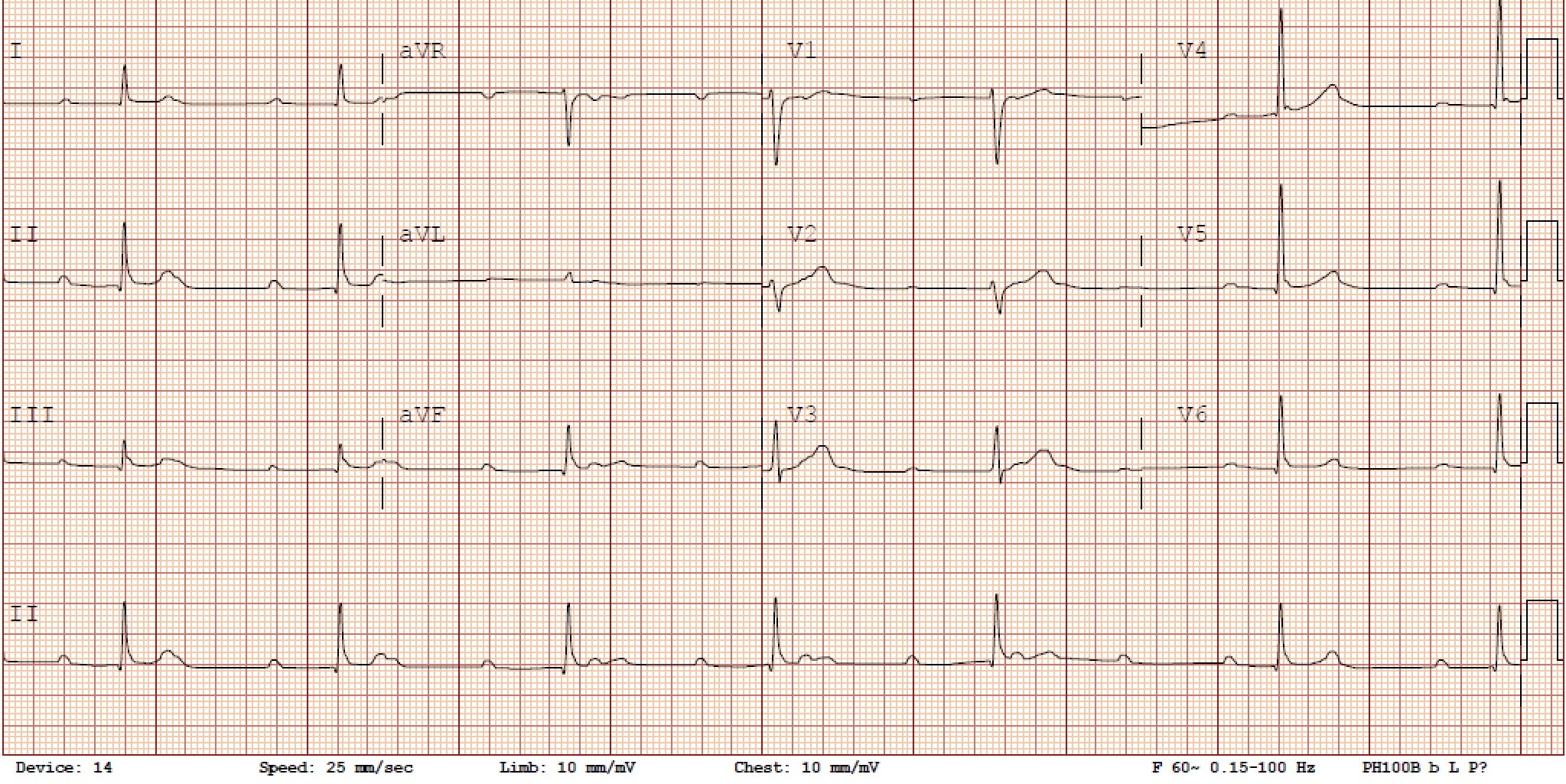
Supplementary material added: Dr Roesler has provided two supplementary standard 12-lead electrocardiograms demonstrating third-degree heart block for additional information: Suppl ECG1, Suppl ECG2. No changes have been made to the article text.
{kind=link}
{kind=link}
This article has been peer reviewed.
 |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. |
References
1. Nelder MP, Wijayasri S, Russell CB, et al. The continued rise of Lyme disease in Ontario, Canada: 2017. Can Commun Dis Rep 2018;44:231-236.
2. Forrester JD, Mead P. Third-degree heart block associated with Lyme carditis: Review of published cases. Clin Infect Dis 2014;59:996-1000.
3. Wan D, Blakely C, Branscombe P, et al. Lyme carditis and high-degree atrioventricular block. Am J Cardiol 2018;121:1102-1104.
4. Fuster LS, Gul EE, Baranchuk A. Electrocardiographic progression of acute Lyme disease. Am J Emerg Med 2017;35:1040.e5-1040.e6.
5. Stanek G, Wormser GP, Gray J, Strle F. Lyme borreliosis. Lancet 2012;379(9814):461-473.
6. Horowitz HW, Sanghera K, Goldberg N, et al. Dermatomyositis associated with Lyme disease: Case report and review of Lyme myositis. Clin Infect Dis 1994;18:166-171.
7. Besant G, Wan D, Yeung C, et al. Suspicious index in Lyme carditis: Systematic review and proposed new risk score. Clin Cardiol 2018;41:1611-1166.
8. Steere AC, Batsford WP, Weinberg M, et al. Lyme carditis: Cardiac abnormalities of Lyme disease. Ann Intern Med 1980;93:8-16.
9. Krause PJ, Bockenstedt LK. Lyme disease and the heart. Circulation 2013;127:e451-e454.
10. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2006;43:1089-1134.
Dr Roesler is a resident physician in the Faculty of Medicine, Department of Dermatology and Skin Science, University of British Columbia. Dr Ephtimios is an infectious diseases physician and medical lead of infectious diseases at the Kelowna Infectious Diseases & Tropical Medicine Clinic and Kelowna General Hospital. He is also a clinical assistant professor of medicine at UBC.