RSV immunization in pregnancy and infancy
Issue: BCMJ,
vol. 67, No. 10, December 2025,
Pages 348-353 Review Articles
ABSTRACT: Respiratory syncytial virus (RSV) is the leading cause of acute respiratory illness in infants, with the highest incidence in the first months of life. In BC, two prevention strategies are available: the adult RSVpreF (Abrysvo) vaccine and the infant monoclonal antibody nirsevimab (Beyfortus). RSVpreF is recommended in BC, but it is not publicly funded. When administered between 32 and 36+6 weeks of gestation (at least 14 days before delivery) to pregnant individuals whose due date falls during or just before the RSV season, the vaccine protects newborns during their highest-risk first 6 months of life. Nirsevimab (Beyfortus) is publicly funded for high- and moderate-risk infants and provides direct protection for an entire RSV season when given once before or during the season. In the future, a universal program combining RSVpreF (Abrysvo) with targeted nirsevimab (Beyfortus) for higher-risk infants could markedly reduce RSV burden across BC, maximizing health benefits with the lowest overall budget impact.
A combined program of universal RSVpreF (Abrysvo) vaccination for pregnant individuals and nirsevimab (Beyfortus) for at-risk infants would substantially curtail respiratory syncytial virus disease burden in BC with the lowest budget impact.
Key points
- Nirsevimab (Beyfortus) is a long-acting monoclonal antibody that provides passive protection against respiratory syncytial virus (RSV) with a single intra-muscular dose per season; it is available in BC from 1 September to 31 March.
- In BC, nirsevimab (Beyfortus) is publicly funded for defined infant populations at increased risk of severe RSV disease, according to provincial eligibility criteria.
- Eligible infants are identified in hospital perinatal units or by public health teams in community settings. Clinicians should verify eligibility and refer through their health authority pathways.
- RSVpreF (Abrysvo) is an adult vaccine approved in pregnancy between 32 and 36+6 weeks of gestation to boost RSV antibody levels at birth and protect infants against severe RSV infections.
- Both immunization products may be available for purchase out-of-pocket or using extended health coverage, with RSVpreF (Abrysvo) priced at approximately $300 and nirsevimab (Beyfortus) at $750.
Background
Respiratory syncytial virus (RSV) is a common seasonal virus and the leading cause of respiratory infections in infants. In British Columbia, RSV cases fall below detection in the summer, increase by late October to early November, and peak from December or January until the end of March.[1] In northern BC, RSV activity is often delayed, peaking in February. Virtually all children are infected by 2 years of age. The risk of severe RSV disease peaks within 3 months of birth.[2] Although most infants recover within a few days, approximately 1% develop bronchiolitis or pneumonia requiring hospitalization.[2]
RSV immunization options
In May 2024, the National Advisory Committee on Immunization recommended that provinces move toward universal infant RSV immunization, prioritizing those at highest risk.[3] Two new passive RSV immunization strategies have become available:
RSVpreF (Abrysvo) is an adult vaccine approved in pregnancy between 32 and 36+6 weeks of gestation.[4-6] It is a recombinant vaccine that stimulates natural antibodies against the RSV fusion protein, which is critical for virus infectivity. The antibodies produced by the pregnant person are then transferred to the fetus via the placenta, which boosts RSV antibody levels at birth and protects infants against severe RSV infections. RSVpreF (Abrysvo) is 57% to 79% effective in reducing RSV hospitalization in infants up to 6 months after birth, when the risk of severe disease is highest.[7-10] Infants born very preterm or with specific chronic conditions involving their heart, lungs, or immune system remain at high risk for longer and require additional protection with nirsevimab (Beyfortus).[2]
Nirsevimab (Beyfortus) is a cell line–produced long-acting human monoclonal antibody that neutralizes RSV by binding to its RSV fusion protein, which prevents virus entry into host cells.[11,12] It is administered directly to the infant and provides protection for at least 6 months from the time of administration.[13] It is not a vaccine and does not induce long-term immunity in the infant. However, in randomized trials and real-world studies, nirsevimab (Beyfortus) reduced medically attended RSV lower respiratory tract illness, RSV hospitalizations, and ICU admissions in first-season infants by approximately 75% to 83%.[14] Nirsevimab (Beyfortus) efficacy against RSV hospitalization remains high for at least 180 days.[15]
Both interventions are available in BC for the 2025–2026 fall/winter season. RSVpreF (Abrysvo) is not publicly funded, but patients may obtain coverage through their private or extended health insurance or the First Nations Health Authority’s Health Benefits Program. The vaccine is also available for $250 to $300, including immunization fees, at local pharmacies. Many community pharmacies carry RSVpreF (Abrysvo).
A publicly funded supply of nirsevimab (Beyfortus) is available for children who meet specific criteria (see “Eligibility criteria,” below). Nirsevimab (Beyfortus) is also available on a private-pay basis (approximately $905 per dose) for children who do not meet the BC RSV program’s eligibility criteria. Private administration requires a prescription and is available only in outpatient settings.
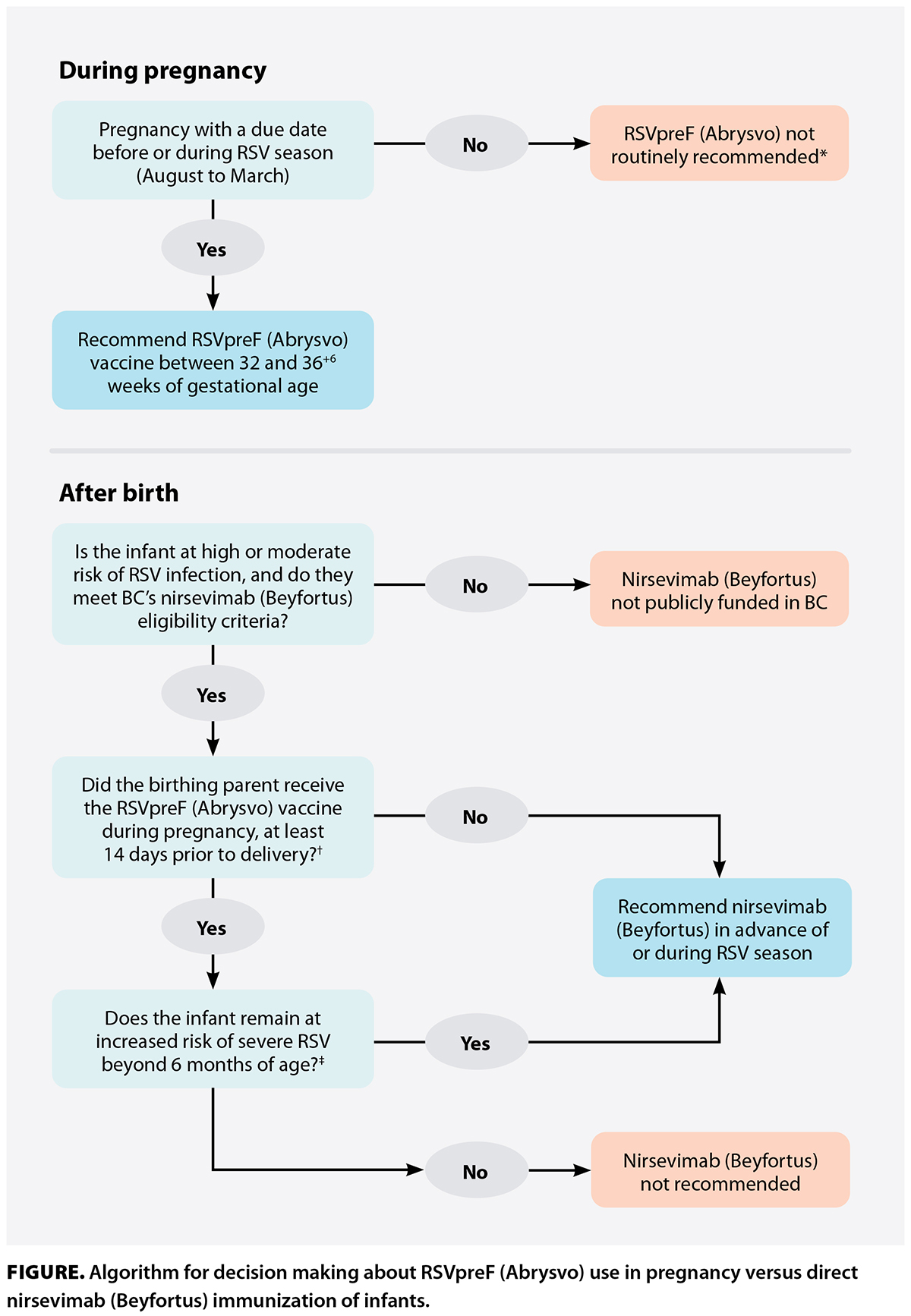 The Figure presents a general algorithm for deciding when RSVpreF (Abrysvo) or nirsevimab (Beyfortus) should be administered. RSVpreF (Abrysvo) is recommended for pregnant individuals from August to March to ensure that the infant is protected during the peak of seasonal RSV activity. Some patients may still choose to get vaccinated with RSVpreF (Abrysvo) outside this period. However, the benefit of RSVpreF (Abrysvo) in the infant beyond 6 months of age is uncertain.
The Figure presents a general algorithm for deciding when RSVpreF (Abrysvo) or nirsevimab (Beyfortus) should be administered. RSVpreF (Abrysvo) is recommended for pregnant individuals from August to March to ensure that the infant is protected during the peak of seasonal RSV activity. Some patients may still choose to get vaccinated with RSVpreF (Abrysvo) outside this period. However, the benefit of RSVpreF (Abrysvo) in the infant beyond 6 months of age is uncertain.
Dual immunization with both products is considered unnecessary for most infants (with exceptions detailed below in “Eligibility criteria”). Providers may consider deferring RSVpreF (Abrysvo) vaccination in select pregnancies where the fetus is affected by a condition that would make the newborn eligible for nirsevimab (Beyfortus) at birth, regardless of maternal vaccination. For example, if the fetus is known to have a trisomy, parents may choose to defer RSVpreF (Abrysvo), as the infant would automatically qualify for nirsevimab (Beyfortus). The combined benefit of both interventions in such cases remains uncertain.
Nirsevimab (Beyfortus)
Efficacy
Nirsevimab (Beyfortus) was first described in 2016.[11] Compared with palivizumab (Synagis), the monoclonal antibody for high-risk infants that was available in BC before fall 2025 and required monthly administration, nirsevimab (Beyfortus) offers two critical improvements: it is 50 times more neutralizing in vitro[11] (about 10 times more neutralizing in vivo[16]), and has a longer half-life in serum (approximately 70 days in infants vs approximately 20–30 days for palivizumab [Synagis]); thus, protection from a single dose of nirsevimab (Beyfortus) lasts for an entire RSV season in BC.[17]
Four RCTs that included more than 12 000 infants demonstrated the safety and efficacy of nirsevimab (Beyfortus) against RSV when administered at the beginning of or during the RSV season (for infants born in season).[17-19] A pooled analysis of the initial three RCTs (Phase 2b, MEDLEY and MELODY trials) indicated that medically attended RSV lower respiratory tract infections and RSV-related hospital admissions were reduced by more than 75%, and severe RSV infection in healthy-term and late-preterm infants was reduced by 86%.[20] Nirsevimab (Beyfortus) recipients also showed a 40% reduction in hospital admissions for any-cause respiratory illness and a 23% reduction in antibiotic prescriptions.[20] Among infants with chronic lung disease, congenital heart disease, or extreme preterm birth, nirsevimab (Beyfortus) serum levels over the first 150 days were similar to those found in the pooled data, indicating a potential extrapolated efficacy to those subpopulations.
During the 2023–2024 RSV season, France, Spain, Luxembourg, and the US implemented universal immunization programs with nirsevimab (Beyfortus) for all infants. Spain achieved very high coverage (approximately 90% to 95%).[21] In contrast, the US faced supply limitations that forced prioritization of high-risk groups as the season progressed.[22] Based on real-world settings, nirsevimab (Beyfortus) resulted in an approximately 80% to 85% reduction in RSV hospitalizations, consistent with clinical trials.[14,23] Considering overall coverage, Catalonia, Spain, achieved approximately 44% to 55% less ED visits for bronchiolitis and approximately 48% to 88% less RSV hospitalizations among infants under 6 months of age.[24] Using our recently published methodology,[2] we estimate that in BC, nirsevimab (Beyfortus) could avert approximately 250 to 300 RSV hospitalizations if all infants were covered under the National Advisory Committee on Immunization’s current recommendations, assuming 80% effectiveness and 90% coverage.[25] For context, approximately 10 000 pediatric hospitalizations of any cause occur each RSV season across the province [unpublished data].
Canadian studies have shown that RSV is associated with substantial pediatric hospital costs.[25-27] Seasonal RSV vaccination for all pregnant individuals, with nirsevimab (Beyfortus) specifically for high- and moderate-risk infants, may be cost-effective compared with a high-risk palivizumab (Synagis) program, whereas a universal nirsevimab (Beyfortus) program for all infants in BC is not cost-effective (at least not without major product cost reductions).[25] A combined program of universal RSVpreF (Abrysvo) vaccination and nirsevimab (Beyfortus) for high- and moderate-risk infants would substantially curtail RSV disease burden in BC, while having the lowest overall budget impact.
Eligibility criteria[28]
Pregnant individuals are recommended to receive the RSVpreF (Abrysvo) vaccine between 32 and 36+6 weeks of gestation, prior to the RSV season, to help protect their infants from severe RSV disease, especially if their baby will still be young (e.g., under 3 months of age) during the peak RSV activity months (December to March).
Infants can receive nirsevimab (Beyfortus) via the publicly funded BC RSV program supply if they meet any of the following criteria and their birthing parent did not receive RSVpreF (Abrysvo):
- Prematurity: Infants born at less than 35 weeks of gestation (i.e., up to 346/7 weeks of gestation).
- Infants with chronic medical conditions involving the heart, lungs, gastrointestinal tract, or nervous system; with severe immunological compromise; or with underlying genetic or metabolic disorders.
- Infants under 6 months of age who live in remote communities, isolated Indigenous communities, or congregate settings such as supportive housing.
Most of these infants do not need nirsevimab (Beyfortus) if RSVpreF (Abrysvo) was given to their birthing parent during pregnancy, unless the baby was born less than 14 days after maternal vaccination (a shorter period between RSVpreF [Abrysvo] vaccination during pregnancy and delivery reduces transplacental antibody transfer).
However, children who remain at high risk of severe RSV disease beyond 6 months of age may receive nirsevimab (Beyfortus) during their first RSV season, regardless of whether their birthing parent received RSVpreF (Abrysvo) during pregnancy, if they are expected to turn 6 months old before the end of the RSV season.
Children with the following conditions remain at increased risk for severe RSV disease beyond 6 months of age and should receive nirsevimab (Beyfortus) during their second RSV season (up to 2 years of age):
- Chronic lung disease requiring ongoing assisted ventilation or oxygen therapy.
- Hemodynamically significant congenital cardiac disease or cardiomyopathy.
- Severe or profound combined immunodeficiencies.
- Severe congenital airway anomalies that impair clearing of respiratory secretions.
- Neuromuscular disease that impairs clearing of respiratory secretions.
- Cystic fibrosis with respiratory involvement and/or growth delay.
- Down syndrome (and other trisomies).
- Preterm infants born at less than 28 weeks of gestation (born after 31 March 2024).
“Children in their second season” generally refers to those of chronological age from 8 months to less than 24 months who have already passed through one period of RSV circulation. However, children who remained hospitalized from birth throughout their first RSV circulation period (e.g., a very premature baby born in January but hospitalized since birth and discharged from the neonatal intensive care unit only in August) are considered to be in their first season upon community discharge, regardless of chronological age.
Ineligibility
Nirsevimab (Beyfortus) provides temporary passive immunity against RSV while the child’s immune system matures. It is not indicated for children 2 years of age or older, as the protection it provides is likely significantly reduced and dosing has not been established over 17 kg. Its administration should be postponed in infants with a moderate or severe acute illness. A mild febrile illness or respiratory infection is not usually a reason to defer immunization. Previous RSV infection is not a contraindication, and eligible infants may still receive nirsevimab (Beyfortus) even after recovering from RSV. It should be used with caution in children with bleeding disorders.
Dosage schedule
In BC, nirsevimab (Beyfortus) is offered from 1 September to 31 March. Infants born before the start of the RSV season should receive their dose in September or October, whereas infants born during the season should get it promptly after birth. Nirsevimab (Beyfortus) is available in 50 mg (0.5 mL) and 100 mg (1 mL) prefilled syringes. Dosage follows a weight-based regimen:
- 50 mg (0.5 mL) if the infant weighs 1.6 kg to less than 5.0 kg.
- 100 mg (1 mL) if the infant weighs 5.0 kg or more.
In BC, reimmunization for a second season is recommended for children up to 2 years of age who have specific conditions (see “Eligibility criteria,” above). These children should receive 200 mg, given as two 100 mg (1 mL) nirsevimab (Beyfortus) injections if they weigh more than 10 kg at the time of dosing.
Infants need only one dose per RSV season, except for children who undergo cardiopulmonary bypass surgery; they should receive a subsequent dose before discharge after the surgery.
Nirsevimab (Beyfortus) can be given with any other routine childhood vaccines. Monoclonal antibodies do not blunt vaccine responses.
All nirsevimab (Beyfortus) doses should be immediately entered in the child’s immunization record after they have been administered. Doses entered in the provincial immunization registry can be viewed in CareConnect, BC’s electronic health record, and by the family using Health Gateway.
Side effects, safety precautions, and contraindications
The adult RSVpreF (Abrysvo) vaccine is contraindicated in individuals with a history of anaphylaxis from the vaccine or any components of the vaccine. Expected side effects include local injection-site reactions, such as pain (41%), redness (7%), and swelling (6%), as well as systemic symptoms, such as myalgias (27%) and fever (3%). It is important to note that only the RSVpreF (Abrysvo) vaccine is indicated in pregnancy; at the time of writing this article, no other RSV vaccines had been approved to be used in pregnancy.
An active vaccine is not yet available for RSV prevention in children. Clinicians should also be aware that RSVpreF (Abrysvo) is indicated only in adults and should not be administered directly to an infant, as it may even produce a deleterious immune response.
Nirsevimab (Beyfortus) is safe for infants. No excess adverse events have been detected in trials that have included more than 12 000 infants.[29] Since its licensure, 500 000 to 2 million infants have received at least one dose, with no major safety concerns.
Based on the product monograph, common reactions include local injection site reactions in 1% of infants and fever and rash in 1% or less of cases.[30] In a Canadian post-licensure safety analysis where parents were asked to report health events within 7 days after nirsevimab (Beyfortus) administration, the main side effect was self-resolving local injection site reactions in approximately 5% of the infants,[31] which, in our clinical experience, resolve quickly. To our knowledge, no cases of anaphylaxis have been reported.
Nirsevimab (Beyfortus) does not appear to delay the risk period for RSV-related hospitalizations in subsequent seasons.[32] Nirsevimab (Beyfortus) is contraindicated in infants with a history of severe allergic reaction to or anaphylaxis from its components (e.g., polysorbate 80) or other humanized monoclonal antibodies.[30]
Referrals and contacts
Infants in BC must meet the BC RSV program’s eligibility criteria to receive publicly funded doses of nirsevimab (Beyfortus). For the 2025–2026 fall/winter season, most eligible infants will likely be identified by hospital programs or public health units. If you think a child may be eligible, please contact your local health authority or public health liaison to coordinate referral and dosing. Email the BC Infant RSV Immunoprophylaxis Program at RSV@cw.bc.ca for any adverse event reporting, cold chain events, or other general inquiries beyond the help and support your health authority can provide.
RSV vaccination in pregnancy
Approximately 10% of infants born in BC are expected to meet the eligibility criteria for nirsevimab (Beyfortus); the remainder rely on the RSVpreF (Abrysvo) vaccine in pregnancy for protection. RSVpreF (Abrysvo) vaccination is recommended for all pregnant individuals unless their infant is expected to qualify for nirsevimab (Beyfortus). The vaccine is available by prescription at many community pharmacies; the BC Pharmacy Association has developed an online map that shows locations that stock it.[33] At present, there is no public funding for the RSVpreF (Abrysvo) vaccine during pregnancy. However, Indigenous individuals covered under the First Nations Health Authority’s Health Benefits Program are eligible to receive the vaccine at no cost, which helps mitigate inequities in access. Additionally, some third-party insurance plans may provide partial coverage.
Other relevant links and references
More information can be found on the BC Centre for Disease Control website, including a detailed Q&A document for BC health care providers.[34] Supporting materials related to RSVpreF (Abrysvo) vaccination in pregnancy and nirsevimab (Beyfortus) immunization in BC are provided on Perinatal Services BC’s Perinatal and Newborn Health Hub.[35]
Competing interests
Dr Wong received a joint ViiV Healthcare and Canadian HIV Trials Network postdoctoral fellowship salary award from 2022 to 2024. The other authors have no competing interests to declare.
This article has been peer reviewed.
 |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. |
@ [YEAR] BC Medical Association
References
1. Viñeta Páramo M, Ngo LPL, Abu-Raya B, et al. Respiratory syncytial virus epidemiology and clinical severity before and during the COVID-19 pandemic in British Columbia, Canada: A retrospective observational study. Lancet Reg Health Am 2023;25:100582. https://doi.org/10.1016/j.lana.2023.100582.
2. Viñeta Páramo M, Watts AW, Bone JN, et al. RSV hospital admissions during the first 2 seasons among children with chronic medical conditions. JAMA Netw Open 2025;8:e2519410. https://doi.org/10.1001/jamanetworkopen.2025.19410.
3. National Advisory Committee on Immunization. Statement on the prevention of respiratory syncytial virus disease in infants. Public Health Agency of Canada, 2024. Accessed 17 October 2025. www.canada.ca/en/public-health/services/publications/vaccines-immunization/national-advisory-committee-immunization-statement-prevention-respiratory-syncytial-virus-disease-infants.html.
4. Wong JMH, Lavoie PM. Respiratory syncytial virus immunization review for prenatal care providers. J Obstet Gynaecol Can 2025;47:103064. https://doi.org/10.1016/j.jogc.2025.103064.
5. Wong JMH, Castillo E, Elwood C, et al. SOGC statement on RSV immunization to prevent infant RSV infection. Society of Obstetricians and Gynaecologists of Canada. July 2024. Accessed 17 October 2025. www.sogc.org/common/Uploaded%20files/Position%20Statements/SOGC%20Statement%20RSV_07182024_EN.pdf.
6. Abu-Raya B, Langley JM, Lavoie PM. Respiratory syncytial virus vaccination in pregnancy. CMAJ 2024;196:E1118-E1119. https://doi.org/10.1503/cmaj.240773.
7. Kampmann B, Madhi SA, Munjal I, et al. Bivalent prefusion F vaccine in pregnancy to prevent RSV illness in infants. N Engl J Med 2023;388:1451-1464. https://doi.org/10.1056/NEJMoa2216480.
8. Simões EAF, Pahud BA, Madhi SA, et al. Efficacy, safety, and immunogenicity of the MATISSE (Maternal Immunization Study for Safety and Efficacy) maternal respiratory syncytial virus prefusion F protein vaccine trial. Obstet Gynecol 2025;145:157-167. https://doi.org/10.1097/AOG.0000000000005816.
9. Gonzalo Pérez M, Vizzotti C, Fell DB, et al. Real-world effectiveness of RSVpreF vaccination during pregnancy against RSV-associated lower respiratory tract disease leading to hospitalisation in infants during the 2024 RSV season in Argentina (BERNI study): A multicentre, retrospective, test-negative, case–control study. Lancet Infect Dis 2025;25:1044-1054. https://doi.org/10.1016/S1473-3099(25)00156-2.
10. Williams TC, Marlow R, Cunningham S, et al. Bivalent prefusion F vaccination in pregnancy and respiratory syncytial virus hospitalisation in infants in the UK: Results of a multicentre, test-negative, case-control study. Lancet Child Adolesc Health 2025;9:655-662. https://doi.org/10.1016/S2352-4642(25)00155-5.
11. Griffin MP, Khan AA, Esser MT, et al. Safety, tolerability, and pharmacokinetics of MEDI8897, the respiratory syncytial virus prefusion F-targeting monoclonal antibody with an extended half-life, in healthy adults. Antimicrob Agents Chemother 2017;61:e01714-e017116. https://doi.org/10.1128/AAC.01714-16.
12. Wilkins D, Yuan Y, Chang Y, et al. Durability of neutralizing RSV antibodies following nirsevimab administration and elicitation of the natural immune response to RSV infection in infants. Nat Med 2023;29:1172-1179. https://doi.org/10.1038/s41591-023-02316-5.
13. Abu-Raya B, Langley JM, Lavoie PM. Nirsevimab to reduce infant morbidity from respiratory syncytial virus. CMAJ 2024;196:E1114-E1117. https://doi.org/10.1503/cmaj.240780.
14. Sumsuzzman DM, Wang Z, Langley JM, Moghadas SM. Real-world effectiveness of nirsevimab against respiratory syncytial virus disease in infants: A systematic review and meta-analysis. Lancet Child Adolesc Health 2025;9:393-403. https://doi.org/10.1016/S2352-4642(25)00093-8.
15. Munro APS, Drysdale SB, Cathie K, et al. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): A randomised, controlled, phase 3b trial. Lancet Child Adolesc Health 2025;9:404-412. https://doi.org/10.1016/S2352-4642(25)00102-6.
16. Wilkins D, Wählby Hamrén U, Chang Y, et al. RSV neutralizing antibodies following nirsevimab and palivizumab dosing. Pediatrics 2024;154:e2024067174. https://doi.org/10.1542/peds.2024-067174.
17. Hammitt LL, Dagan R, Yuan Y, et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med 2022;386:837-846. https://doi.org/10.1056/NEJMoa2110275.
18. Drysdale SB, Cathie K, Flamein F, et al. Nirsevimab for prevention of hospitalizations due to RSV in infants. N Engl J Med 2023;389:2425-2435. https://doi.org/10.1056/NEJMoa2309189.
19. Griffin MP, Yuan Y, Takas T, et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med 2020;383:415-425. https://doi.org/10.1056/NEJMoa1913556.
20. Simões EAF, Madhi SA, Muller WJ, et al. Efficacy of nirsevimab against respiratory syncytial virus lower respiratory tract infections in preterm and term infants, and pharmacokinetic extrapolation to infants with congenital heart disease and chronic lung disease: A pooled analysis of randomised controlled trials. Lancet Child Adolesc Health 2023;7:180-189. https://doi.org/10.1016/S2352-4642(22)00321-2.
21. Trusinska D, Lee B, Ferdous S, et al. Real-world uptake of nirsevimab, RSV maternal vaccine, and RSV vaccines for older adults: A systematic review and meta-analysis. EClinicalMedicine 2025;84:103281. https://doi.org/10.1016/j.eclinm.2025.103281.
22. Centers for Disease Control and Prevention Health Alert Network. Limited availability of nirsevimab in the United States—Interim CDC recommendations to protect infants from respiratory syncytial virus (RSV) during the 2023–2024 respiratory virus season [health advisory]. 23 October 2023. Accessed 3 April 2025. www.cdc.gov/han/2023/han00499.html.
23. Assad Z, Romain A-S, Aupiais C, et al. Nirsevimab and hospitalization for RSV bronchiolitis. N Engl J Med 2024;391:144-154. https://doi.org/10.1056/NEJMoa2314885.
24. Perramon-Malavez A, Buonsenso D, Morello R, et al. Real-world impact of nirsevimab immunisation against respiratory disease on emergency department attendances and admissions among infants: A multinational retrospective analysis. Lancet Reg Health Eur 2025;55:101334. https://doi.org/10.1016/j.lanepe.2025.101334.
25. Moradpour Taleshi J, Viñeta Páramo M, Watts A, et al. Cost-effectiveness of infant and maternal RSV immunization strategies. In press. medRxiv 2025. Accessed 17 October 2025. https://doi.org/10.1101/2025.06.27.25330432.
26. Shoukat A, Abdollahi E, Galvani AP, et al. Cost-effectiveness analysis of nirsevimab and maternal RSVpreF vaccine strategies for prevention of respiratory syncytial virus disease among infants in Canada: A simulation study. Lancet Reg Health Am 2023;28:100629. https://doi.org/10.1016/j.lana.2023.100629.
27. Gebretekle GB, Yeung MW, Ximenes R, et al. Cost-effectiveness of RSVpreF vaccine and nirsevimab for the prevention of respiratory syncytial virus disease in Canadian infants. Vaccine 2024;42:126164. https://doi.org/10.1016/j.vaccine.2024.126164.
28. Provincial Health Services Authority. 2025–2026 provincial infant RSV program eligibility criteria. 11 June 2025 (revised October 24, 2025). Accessed 24 October 2025. https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-06-63004.pdf.
29. Mankad VS, Leach A, Chang Y, et al. Comprehensive summary of safety data on nirsevimab in infants and children from all pivotal randomized clinical trials. Pathogens 2024;13:503. https://doi.org/10.3390/pathogens13060503.
30. AstraZeneca Canada Inc. BeyfortusTM nirsevimab injection. 19 April 2023. Accessed 17 October 2025. https://pdf.hres.ca/dpd_pm/00070439.PDF.
31. Viñeta Páramo M, Kiely M, Valiquette L, et al. Post-licensure safety of nirsevimab from the Canadian National Vaccine Safety (CANVAS) network. medRxiv 2025. Under review. Accessed 17 October 2025. https://doi.org/10.1101/2025.08.14.25333604.
32. Coma E, Martínez-Marcos M, Hermosilla E, et al. Impact of nirsevimab immunoprophylaxis on respiratory syncytial virus-related outcomes in hospital and primary care after two consecutive seasons: A population-based retrospective cohort study in infants in their second year of life in Catalonia, Spain. Eur J Pediatr 2025;184:616. https://doi.org/10.1007/s00431-025-06440-x.
33. British Columbia Pharmacy Association. Respiratory syncytial virus (RSV) vaccines in pharmacies. Accessed 17 October 2025. www.bcpharmacy.ca/rsv-vaccines.
34. BC Centre for Disease Control. BC Infant Respiratory Syncytial Virus (RSV) Immunoprophylaxis Program questions and answers for immunization providers. Updated September 2025. Accessed 17 October 2025. www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Guidelines%20and%20Manuals/Immunization/Vaccine%20Info/RSV_Nirsevimab_HCP_QA.pdf.
35. Provincial Health Services Authority, Perinatal Services BC. 2025–2026 infant RSV immunoprophylaxis program updates now available. Perinatal and Newborn Health Hub. 12 September 2025. Accessed 17 October 2025. www.psbchealthhub.ca/alerts-and-updates/991.
Dr Viñeta Páramo is a PhD candidate in the Women+ and Children’s Health Sciences program at the University of British Columbia. Dr Wong is an obstetrician and gynecologist and reproductive infectious diseases specialist at BC Women’s Hospital and Health Centre and at St. Paul’s Hospital. Dr Lavoie is a neonatologist at BC Women’s Hospital and Health Centre and medical director of the BC Infant RSV Immunoprophylaxis Program.
Corresponding author: Dr Pascal Lavoie, plavoie@cw.bc.ca.
