Mild traumatic brain injury and psychiatric illness
Psychiatric illness, particularly depression, has an increased incidence following mild traumatic brain injury, possibly as a result of damage to the frontal lobes. This damage may also lead to personality change and attentional problems. A number of treatment options, including psychotherapy and the use of medications, should be considered.
Psychiatric illness, particularly depression, is common after brain injuries, but there are a number of treatments we can use to help these patients.
Lishman[1] was one of the first authors to note the association between traumatic brain injury and the development of psychiatric disorders. It is not surprising that there would be an increased risk of these types of diagnoses following a traumatic brain injury, since the parts of the brain most susceptible to damage from trauma are the frontal and the parietal lobes, which are also known to be the location of most psychiatric disorders.
It is generally accepted that the incidence of psychiatric illness and other neurobehavioral difficulties increases with the severity of traumatic brain injury. The primary care physician should be alert to the possibility of psychiatric illness in brain-injured patients and be prepared to assess, treat, and refer as necessary.
Depression is by far the most common psychiatric sequela following traumatic brain injury, with reported prevalence “ranging over 50%.”[2] Furthermore, patients are at risk for developing depression not only in the acute phase but for decades after the injury, when their risk remains elevated.
Jorge and colleagues[3] noted major depression in 33% of 91 patients who had sustained a traumatic brain injury. They also noted comorbid anxiety in 76.7% and aggressive behavior in 56.7%. Forty of their patients had sustained a mild traumatic brain injury (mTBI), with the rest having moderate and severe injuries. Mah and colleagues[4] found deficits in social perception after damage to the orbital frontal cortex. These changes interfered with the patients’ ability to accurately evaluate emotional facial expressions.
Recently, Levin and colleagues[5] studied a cohort of 125 adults with mild traumatic brain injury. Reviewing their own earlier work, they cited an incidence of major depression of 17% in individuals with mild traumatic brain injury 1 year postinjury. In their more recent work, they noted an increasing incidence of depression based on age, and that incidence increased by a factor of 7, depending on whether there were abnormal CT findings on brain imaging.
The differential diagnosis of depressive symptomatology following a brain injury includes the following:
• Adjustment disorder with depressed mood
• Apathy and emotional lability due to frontal lobe syndrome
• Dysthymia
• Major depression
If it is determined that the depression or mood disorder is secondary to brain injury, it should be recorded using DSM-IV-TR as “a mood disorder due to a general medical condition (brain injury).”
Screening for depressive illness can be done using clinical interview or any standard checklists such as the Hamilton or Beck Depression Inventory.
The treatment of depressive illness following mTBI is generally the same as for mood disorders not related to trauma. Because injured individuals may be suffering pain as well as a psychiatric disorder, particular attention needs to be paid to treating problems with sleep secondary to pain as part of the overall approach to mood disturbance and psychiatric disorders in general.
Moldover and colleagues[2] have recently argued that depression represents a heterogeneous category with multiple etiological pathways. They present suggestions on differential diagnosis and treatment options.
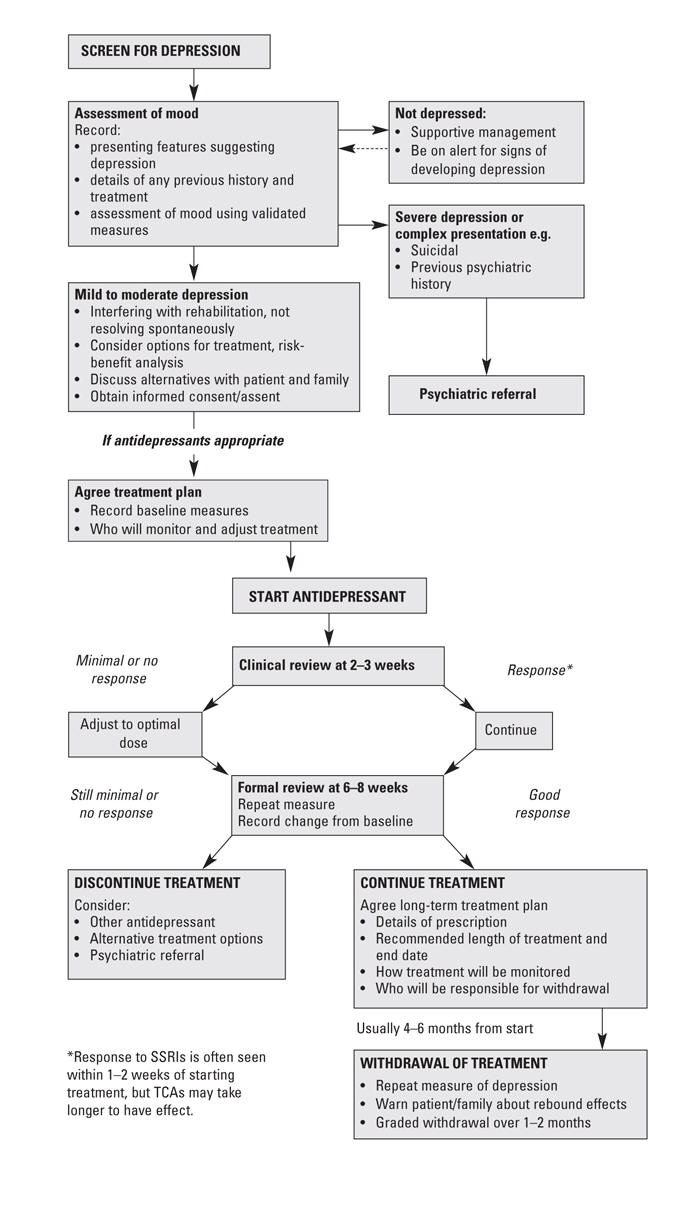
One of the most practical recent publications is by Turner-Stokes and MacWalter, who present guidelines for screening, assessing, and treating depression in the context of brain injury. They also provide guidance regarding how to monitor and evaluate treatment, and when to refer for formal psychiatric review. A more detailed review by the same authors is available as part of the British National Guidelines project. A number of reproducible practical tools, including information sheets for patients, are included. The flow chart in the accompanying Figure is one of these tools.
It is accepted that bipolar disorder after brain injury is extremely rare. Sayal and colleagues[7] describe a case of bipolar injury following mTBI with small lesions in the right amygdala, right putamen, and right of the pituitary gland.
Treatment of all of these disorders borrows on treatment protocols developed for individuals who are not brain injured. There are, however, no controlled trials of either psychotherapy or medications specific to the brain-damaged population.
Psychoeducational approaches and supportive psychotherapy will benefit patients in the acute stages of recovery from their injuries. Cognitive-behavioral therapy is probably the treatment of choice, although it must be remembered that cognition may have been adversely affected by the brain injury itself. Serotonin reuptake inhibitor antidepressants are the medications of choice.
The five major anxiety disorders described in DSM-IV-TR (generalized anxiety disorder, social anxiety disorder, posttraumatic stress disorder, obsessive-compulsive disorder, and panic disorder) all have increased rates following brain trauma. The disorder may be due directly to the brain injury itself, or be secondary to the life experiences that are associated with the trauma. In some cases the disorder can be specific to a lesion in the brain. This is particularly the case with obsessive-compulsive disorder, which is associated with certain subcortical lesions.
Posttraumatic stress disorder (PTSD) involves the re-experiencing of memories associated with the trauma. Therefore, individuals who suffer a dense amnesia at the time of the trauma have some, but not absolute, protection against developing PTSD. Since individuals with mTBI have relatively shortened periods of amnesia associated with the trauma, PTSD is more common in individuals with mTBI than with severe brain injury.
Hiott and Labbate[8] have reviewed anxiety disorders following traumatic brain injury. They report a number of studies with high incidence of PTSD, but note that the re-experiencing criteria were largely accounted for by the emotional reactivity criteria and not by the current or distressing recollections or dreams of the event.
Neuroimaging studies in PTSD have implicated the amygdala, hippocampus, and other limbic structures. Injury to these parts of the brain may actually predispose individuals to developing PTSD or other anxiety disorders.
Grados[9] has recently reviewed the diagnosis and treatment of anxiety disorders following traumatic brain injury, particularly obsessive-compulsive disorder. Much of the literature revolves around case reports. Grados states that obsessive-compulsive phenomena following brain injury are probably more common than generally expected. Most symptoms have an early onset.
Psychosis following traumatic brain injury
Psychosis more typically develops after severe brain injuries, but has been reported after relatively mild traumatic brain injury. Arciniegas and colleagues[10] provide a full differential diagnosis for posttraumatic psychosis as well as treatment guidelines. Generally speaking, antipsychotic medication should be prescribed, beginning with one-third to one-half the starting dose used in psychiatric patients who are not brain injured.
McAllister and Ferrell[11] have noted a connection between the development of psychotic features and orbital frontal, temporal, and basal ganglion damage following mTBI. They also provide a good set of treatment guidelines. They recommend treatment with the standard neuroleptic medications, risperidone, olanzapine, and quetiapine.
Alteration in personality is frequently reported by families as the most troublesome sequela of a brain injury. It is probable that changes in personality are part of the frontal lobe syndrome, arising from direct damage to the frontal lobes. Disinhibited symptoms are frequently seen following damage to the orbital frontal area, disorganized syndromes following damage to the dorsal lateral region, and apathetic personalities following damage to the medial frontal region. Establishing change in personality following posttraumatic brain injury relies heavily on collateral information from relatives concerning how the patient was prior to the injury. Patients themselves may not have much insight into subtle alterations in their personality.
These changes would be documented under the DSM-IV-TR category “personality change due to a general and medical condition.” DSM-IV-TR lists a variety of subtypes, including labile, disinhibited, aggressive, apathetic, paranoid, and mixed presentations.
Individuals with alterations in personality due to brain injury are relatively resistant to treatment.
There are a variety of symptoms frequently seen in individuals who have suffered concussion or mTBI, including fatigue, disordered sleep, headache, dizziness, irritability or aggression, affective lability, changes in personality, and apathy or lack of spontaneity. These features are referenced in the DSM-IV-TR discussion of postconcussion disorder, but the disorder itself is not included as an official diagnosis because of insufficient information to warrant it. Although these symptoms are frequently seen following concussion or mild traumatic brain injury, they are also common in the general population and in trauma victims who have not suffered brain damage or concussion.
A full discussion of this medical controversy was recently reviewed by Rees,[12] who recommends abandoning the term “persistent postconcussive syndrome.”
The vast majority of individuals with mild traumatic brain injury have resolution of these symptoms by 3 months. In a large study of concussed athletes, all subjects had total resolution of these symptoms by 3 months and in most cases by 7 days.[13]
It is common to find individuals with changes in their cognitive abilities following traumatic brain injury. Changes are frequently reported with attention, memory, and executive function. Intelligence per se is relatively resistant to brain trauma and is unlikely to be affected by mild traumatic brain injury. The role of the general practitioner or psychiatrist is to identify cognitive changes and to make an appropriate referral to a neuropsychologist for documentation of these problems.
Problems in attention following mild traumatic brain injury have recently been described as “secondary attention-deficit hyperactivity disorder.” Specific instruments for measuring attention following mTBI are not fully developed. In the absence of better instruments, tools used for assessing and diagnosing attention-deficit hyperactivity disorder in children and adults should be used if attentional problems are identified following mild traumatic brain injury. Affected individuals may do poorly on the digit span of the Wechsler Intelligence Scale for Children (WISC) or the Wechsler Adult Intelligence Scale (WAIS).
Treatment of inattention using psychostimulants is increasingly recognized as beneficial. Standard doses of methylphenidate and dextroamphetamine have been shown to benefit patients with attentional problems, while the longer-acting preparations Adderall-XR (dextroamphetamine) and Concerta (methylphenidate) are the current medications of choice since they are taken once a day and last for 12 hours, thereby enhancing compliance.
Disturbances in sleeping are commonly seen in both mood and anxiety disorders. Furthermore, one of the most common presentations following trauma, particularly motor vehicle trauma, is the development of pain leading to sleep disorders and then resulting in a mood disturbance. Poor sleep can also negatively affect cognition, so addressing problems with sleep is critically important in dealing with a patient with a brain injury.
There are no controlled trials dealing with sleep disorders following traumatic brain injury, so clinicians need to rely on treatment strategies derived from the study of sleep disorders in general. Patients should be advised to follow accepted rules of sleep hygiene, such as going to bed and getting up at a specific time, engaging in relatively vigorous exercise on a regular basis, and avoiding the use of coffee and other stimulants later in the evening. The benzodiazepines and other sedative hypnotics such as zopiclone can help patients sleep in the short term; however, for long-term treatment, particularly in the presence of mood disorders, there is better evidence supporting the use of sedating antidepressants such as trazodone and amitriptyline. Melatonin, an over-the-counter preparation currently available in British Columbia, has been known to be effective in a wide variety of sleep disorders. Doses range from 1.5 to 24 mg.
Lee and colleagues[14] have published on the treatment of psychiatric disorders secondary to brain injury. They note that there is a lack of research-based evidence in the brain-injured population. They do recommend, however, that clinicians start low and go slow, that there be a continuous reassessment of the clinical condition, and that augmentation strategies be developed for partial response. They provide specific treatment guidelines for all of the conditions discussed in this article. A summary of the medications they recommend appears in the accompanying Table.
Following mild traumatic brain injury, there is an increased risk of patients developing standard psychiatric disorders, specific alterations in personality function, and cognitive difficulties, particularly regarding attention. All of these conditions require assessment and effective treatment in the first instance by the primary care physician. Many cases will necessitate a referral to a psychiatrist for assessment and treatment.
Competing interests
None declared.
References
1. Lishman WA. Organic Psychiatry: The Psychological Consequences of Cerebral Disorder. 3rd ed. Malden, MA: Blackwell Science; 1998. 922 pp.
2. Moldover J, Goldberg KB, Prout MF. Depression after traumatic brain injury: A review of evidence for clinical heterogeneity. Neuropsychol Rev 2004;14:143-154. PubMed Abstract Full Text
3. Jorge RE, Robinson RG, Moser D, et al. Major depression following traumatic brain injury. Arch Gen Psychiatry 2004;61:42-50. PubMed Abstract Full Text
4. Mah L, Arnold MC, Grafman A. Impairment of social perception associated with lesions of the prefrontal cortex. Am J Psychiatry 2004:161:1247-1255. PubMed Abstract Full Text
5. Levin HS, McCauley SR, Josic CP, et al. Predicting depression following mild traumatic brain injury. Arch Gen Psychiatry 2005;62:523-528. PubMed Abstract Full Text
6. Turner-Stokes L, MacWalter R; Guideline Development Group of the British Society of Rehabilitation Medicine; British Geriatrics Society; Royal College of Physicians London. Use of antidepressant medication following acquired brain injury: Concise guidance. Clin Med 2005;5:268-274. PubMed Abstract Full Text
7. Sayal K, Ford T, Pipe R. Case study: Bipolar disorder after head injury. J Am Acad Child Adolesc Psychiatry 2000;39:525-528. PubMed Abstract Full Text
8. Hiott DW, Labbate L. Anxiety disorders associated with traumatic brain injuries. NeuroRehabilitation 2002;17:345-355. PubMed Abstract Full Text
9. Grados M. Obsessive-compulsive disorder after traumatic brain injury. Int Rev Psychiatry 2003;15:350-358. PubMed Abstract Full Text
10. Arciniegas DB, Harris SN, Brousseau KM. Psychosis following traumatic brain injury. Int Rev Psychiatry 2003;15:328-340. PubMed Abstract Full Text
11. McAllister TW, Ferrell RB. Evaluation and treatment of psychosis after traumatic brain injury. NeuroRehabilitation 2000;17:357-368. PubMed Abstract Full Text
12. Rees PM. Contemporary issues in mild traumatic brain injury. Arch Phys Med Rehabil 2003;84:1885-1894. PubMed Abstract Full Text
13. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects and recovery time following concussion in collegiate football players: The NCAA Concussion Study. JAMA 2003;290:2556-2563. PubMed Abstract Full Text
14. Lee HB, Lyketsos CG, Rao V. Pharmacological management of the psychiatric aspects of traumatic brain injury. Int Rev Psychiatry 2003;15:359-370. PubMed Abstract Full Text
Derryck H. Smith, MD, FRCPC
Dr Smith is head of the Department of Psychiatry at Children’s and Women’s Health Centre in Vancouver, BC, and a clinical professor in the Department of Psychiatry at the University of British Columbia. He also serves on the Review Panel of the Ontario Neurotrauma Foundation.

{kind=link}