Meningococcal disease in British Columbia—2001 summary
Issue: BCMJ,
vol. 44 , No. 4 , May 2002 ,
Pages 203-210 Clinical Articles
Sixty cases of laboratory-confirmed meningococcal disease were reported in British Columbia in 2001—the highest number since 1985. Serogroup C was responsible for 47% of cases, with 15- to 29-year-old youths having the highest rate of serogroup C disease. A serogroup C outbreak in the Abbotsford area affecting this age group was successfully controlled by a vaccination campaign using a newly licensed protein-conjugate meningococcal C vaccine. Availability of polymerase chain reaction testing through BC’s Children’s and Women’s Health Centre and molecular testing at the BC Centre for Disease Control have increased diagnostic sensitivity and specificity of meningococcal disease. If routine childhood immunization using a conjugate C vaccine was implemented, community serogroup C outbreaks could be eliminated. Until a public program is approved, meningococcal vaccine may be privately purchased through pharmacies or travel clinics.
A summary of meningococcal disease surveillance for British Columbia during 2001, background information about the disease, and a summary of current public health recommendations, including immunization.
In 2001, meningococcal disease re-emerged as one of the most significant public health issues in British Columbia. Highlights included:
• A significant increase in overall provincial meningococcal disease activity.
• An outbreak of serogroup C meningococcus in the Abbotsford area that was successfully controlled using a new conjugate-protein meningococcal C vaccine.
• Introducing important laboratory enhancements for diagnosis and molecular evaluation of meningococcus.
• Expanding public health guidelines for who contact tracing and prophylaxis are recommended, to include cases of primary meningococcal conjunctivitis and pneumonia.
• A recommendation by the provincial health officer, the British Columbia Centre for Disease Control, and provincial Communicable Disease Policy Committee that the Ministry of Health Services implement a routine meningococcal immunization program for all children 1 year of age, in addition to youths in grades 6 and 9, using a conjugate meningococcal C vaccine.
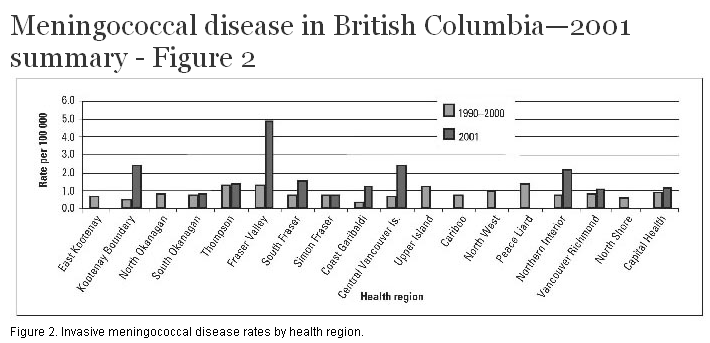
Sixty laboratory-confirmed cases of meningococcal disease were reported in British Columbia during 2001—the highest number reported in any year since provincial meningococcal disease surveillance began in 1985. Fifty-three of these were invasive presentations (mainly meningitis and/or septicemia), representing an incidence rate of invasive meningococcal disease of 1.3 per 100 000, 44% above the average British Columbia incidence rate over the previous decade of 0.9 per 100 000 (Figure 1 and Figure 2). The remaining seven cases were non-invasive presentations (pneumonia and conjunctivitis).
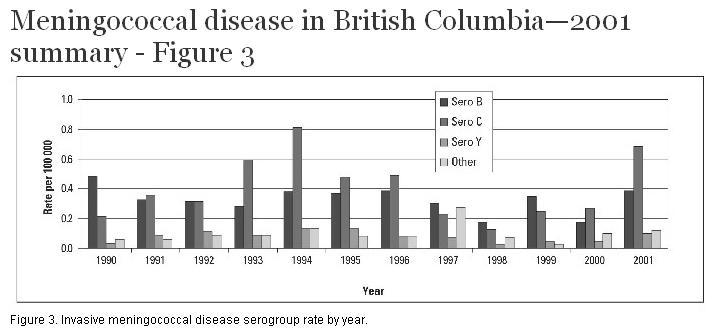
Serogroups C and B were responsible for 28 of 60 (47%) and 19 of 60 (31%) cases respectively of laboratory-confirmed meningococcal disease. Seven cases (12%) were either not serogroupable or did not have serogroup data available, while four (7%) were serogroup Y and two (3%) serogroup W-135. The distribution of serogroups in 2001 did not vary significantly from the provincial historic average since 1990, over which time serogroups C and B comprised 43% and 37% of laboratory-confirmed meningococcal disease cases (Figure 3).
Overall case fatality rate for invasive meningococcal disease in 2001 was 11%, up from an average 9% over the previous decade. For serogroup C disease the case fatality rate for 2001 was 21%, a 50% increase compared with the average 14% observed for this serogroup since 1990.
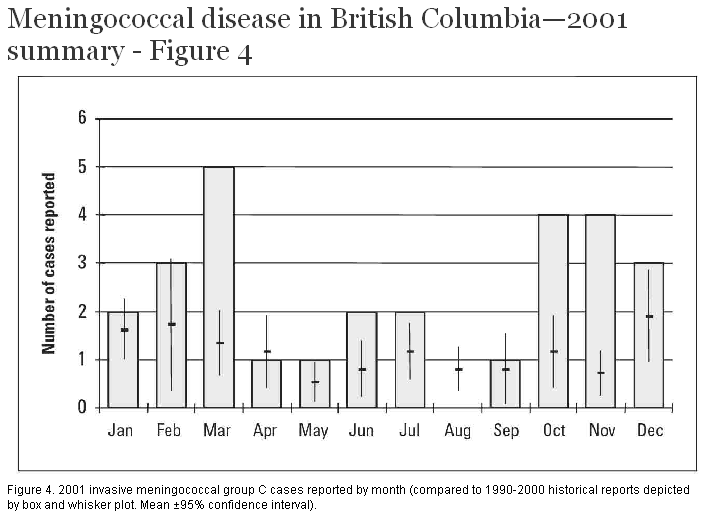
The overall rate of reported serogroup C disease in British Columbia in 2001 was 0.7 per 100 000, 75% above the average historic (1990–2000) rate of 0.4 per 100 000 (Figure 4). Fourteen of 28 (50%) serogroup C cases were in the age group 15 to 29 years, corresponding to a rate of 1.7 per 100 000 for this age group—2.4 times higher than the overall population rate.
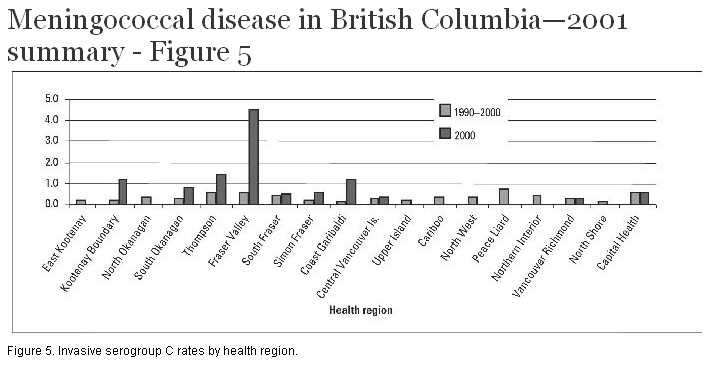
The primary reason for the increased rate of serogroup C disease in British Columbia and among older teens and young adults was an outbreak in Abbotsford/Mission during 2001 (Figure 5). Seven of 14 (50%) of all serogroup C cases in British Columbia occurring in 15- to 29-year-olds during 2001 were reported from the Abbotsford area. Overall, 11 of 28 (39%) of serogroup C cases reported in British Columbia were from the Abbotsford area, which experienced a serogroup C rate of 9.3 per 100 000—23 times higher than the 2001 rate of serogroup C disease for the rest of the province. By contrast, the 2001 rate of serogroup C disease in the rest of BC—0.4 per 100 000—was the same as the average, historic provincial rate, with 17 cases of serogroup C disease scattered across nine other health service delivery areas throughout BC.
In the Abbotsford area, a public health meningococcal immunization campaign was undertaken between April and October 2001. Based on the age range and other epidemiologic features of reported cases, the group targeted for vaccination was 19- to 29-year-olds who live, work, or study in Abbotsford and Mission, as well as high school-aged students in Abbotsford and salivary contacts of the affected group. Quebec and British Columbia were the first jurisdictions in North America to use a conjugate meningococcal C vaccine for outbreak control. Approximately 40 000 doses of meningococcal vaccine were distributed and an estimated 90% of high school students, and 70% of other eligible members of the target group were immunized. No instances of vaccine failure and only a few, non-severe adverse reactions were reported.
In conjunction with this immunization campaign, a study was undertaken to assess the prevalence and serogroup distribution of meningococcus in the group targeted for immunization and among younger and older persons. The overall nasopharyngeal carriage rate of meningococcus was 8%, but for serogroup C was only 0.3% (3 per 1000) and for the clone of serogroup C responsible for the outbreak, only 0.1% (1 per 1000).[1] This study supported a hypothesis that a more virulent meningococcal clone was primarily responsible for the increased risk of invasive disease observed in Abbotsford, despite a low nasopharyngeal prevalence, even within the high-risk population targeted for immunization.
Subsequently, four additional cases of serogroup C disease occurred in persons residing in the Abbotsford area. They were older than the immunized group, and three had direct or indirect links with the community street-oriented population. A focused immunization campaign targeting persons with this profile was successfully undertaken in December in Abbotsford, with approximately 150 people immunized. As of March 2002, these public health interventions have successfully controlled the Abbotsford serogroup C outbreak.
The 19 cases of serogroup B reported in British Columbia in 2001 correspond to a rate of serogroup B disease of 0.5 per 100 000, 67% above the average historic (1990–2000) rate of 0.3 per 100 000. Serogroup B disease has been clustered in four health regions, which reported 17 of the 19 cases: South Fraser (five cases), Central Vancouver Island (four cases), Vancouver (five cases), and Capital Region (three cases). Consistent with historic trends, the highest rate of serogroup B disease in 2001 (2.4 per 100 000) occurred in infants less than 1 year of age. However, this was based on only one case among infants, and in fact was below the average historic provincial rate of serogroup B disease among infants of 7 per 100 000. Serogroup B cases were reported across a wide age range, up to 82 years of age.
During 2001, serogroup Y disease continued to be reported at a very low rate (one per million) and continues to represent a low proportion of all reported laboratory-confirmed meningococcal disease (7%) in British Columbia. This is at variance to increasing rates of serogroup Y disease in Ontario and the United States, where serogroup Y comprises more than 30% of all reported meningococcal disease.[2,3]
Laboratory enhancements in diagnosis and molecular evaluation of meningococcus
During 2000–01, through a joint initiative of BC’s Children’s and Women’s Health Centre and the BC Centre for Disease Control (BCCDC), polymerase chain reaction (PCR) nucleic acid testing became available as a diagnostic tool for meningococcus in British Columbia.[4] The increased diagnostic sensitivity of PCR, particularly in a setting of antibiotic use prior to specimen collection, resulted in the laboratory confirmation of 11 cases of invasive disease that could not be confirmed by culture or antigen testing.[5] This represents a 24% increase in diagnostic sensitivity of invasive meningococcal disease over traditional culture or latex antigen testing methods (BC Centre for Disease Control, unpublished data, 2002). The recent implementation of pulse field gel electrophoresis testing of meningococcal isolates at BCCDC enables better characterization of molecular epidemiologic aspects of meningococcal disease. For example, molecular study of invasive serogroup C meningococcal isolates revealed a unique clone of meningococcus associated with the Abbotsford outbreak and corroborated evidence from case surveillance that the focus of increased serogroup C activity had remained geographically restricted to the Abbotsford area during 2001.
Current meningococcal vaccines
Polysaccharide meningococcal vaccines
Polysaccharide vaccines are available in Canada for protection against serogroups A, C, Y, and W-135. These vaccines provide good protection (about 80%) in older teens and healthy adults but are less effective in children under 10 years of age.[6,7] They are not generally recommended for children under 2 years of age, except for protection against serogroup A disease.[8] The duration of protection is generally short, and booster doses are recommended at 3- to 5-year intervals for those at ongoing risk.[8]
Conjugate meningococcal C vaccines
Two conjugate meningococcal C vaccines were licensed in Canada in 2001: Menjugate (Chiron Corp), and Neis Vac-C (Shire Biochem). Licensure of a third (similar) product, Mengitec (Wyeth-Ayerst Canada) is anticipated in early 2002. Unlike polysaccharide meningococcal vaccines, these products are highly effective in young children and infants as young as 2 months of age.[8] These products have been used in highly successful immunization campaigns for children 2 months to 20 years of age in the United Kingdom[9] and Quebec (P. DeWals, MD, Université de Sherbrooke, oral communication, February 2002). In both cases, wide-scale meningococcal C outbreaks were rapidly controlled with mass childhood immunization. Evidence to date suggests that these vaccines provide longer-term, boostable individual protection of at least 5 years’ duration,[10] and may potentially offer indirect protection of unimmunized persons (herd immunity) if population vaccine uptake is sufficiently high to reduce community transmission.[11]
Currently in British Columbia, publicly funded meningococcal immunization is provided for those at high risk of invasive disease, including persons with an absent or poorly functioning spleen, persons requiring bone-marrow transplant, and those with certain types of immune deficiency. Although not publicly funded, meningococcal immunization should also be considered in other circumstances, such as higher-risk international travel, on the recommendation of a travel medicine consultant.[12] No known cases of vaccine-preventable (serogroups A, C, Y, W-135) meningococcal disease were reported among college or university-attending students in British Columbia during 2001, and the risk of invasive meningococcal disease in this setting appears to be low in the province. Meningococcal serogroup C outbreaks in this setting have occurred elsewhere however, and in the United States, freshmen, particularly those living in dormitories, have a modestly increased risk of meningococcal disease.[13] British Columbia post-secondary students, especially first-year students living in dormitories, are encouraged to consider meningococcal immunization.
Routine meningococcal immunization program recommended for British Columbia
In 2001, Canada’s National Advisory Committee on Immunization (NACI) made a recommendation that all children up to 5 years of age, teenagers, and young adults be immunized against meningococcal C disease using conjugate meningococcal C vaccine.[8] The provincial health officer, BCCDC, and provincial Communicable Disease Policy Committee have recommended that British Columbia implement a routine, province-wide, meningococcal immunization program for all children 1 year of age, in addition to youths in grades 6 and 9, using a conjugate meningococcal C vaccine. Such a program would eliminate meningococcal C outbreaks, which have occurred about every 2 to 3 years in British Columbia over the past decade, and reduce the burden of serogroup C disease by at least 75% in the first 15 years, preventing approximately 100 cases and 15 deaths over this time period (BC Centre for Disease Control, unpublished data, 2001).
Private purchase option for conjugate meningococcal C vaccine
Individuals wishing to protect their children or themselves against meningococcal C disease can privately purchase either Menjugate or Neis Vac-c. Meningococcal vaccines can be purchased without a prescription from any pharmacy in BC (J. Seto, BCCDC, written communication, March 2002). Vaccines should be transported and stored at a temperature between 2°C to 8°C, so persons purchasing vaccine should bring an insulated container with ice to pick up the product and preferably take it directly to their physician’s office for storage/administration. The list retail prices for Menjugate and Neis Vac-C are approximately $89 and $79 per dose respectively (J. Seto, BCCDC, oral communication, March 2002). Both are safe and highly effective vaccines.[14-17]
Background information about meningococcal disease
Meningococcal disease is caused by the bacterium Neisseria meningitidis, also referred to as meningococcus. There are several different strains of meningococcus, categorized into serogroups. Serogroups A, B, C, W-135, and Y are the most common serogroups affecting humans. This organism is generally a harmless, transient inhabitant of the nose and throat of healthy people, where it will typically persist for periods ranging from weeks to months. Rarely, meningococcus will invade the blood, lining of the brain, or other normally sterile body tissues, causing invasive disease. Meningococcus is passed person-to-person by direct contact with an infected person’s saliva or respiratory secretions. Thus, good personal hygiene, such as hand washing and avoiding sharing items such as lipstick and cigarettes, may reduce personal risk. Large-scale outbreaks may occur sporadically, or seasonally, such as during the dry season of sub-Saharan Africa.[18] In British Columbia, most meningococcal disease occurs as random, single cases.
At any one time, between 10% and 20% of healthy people (corresponding to between 400000 and 800000 people in British Columbia), will be harmlessly carrying meningococcus in their nose or throat.[19,20] Over a period of a year, possibly 1 to 2 million people in British Columbia will have at one point been infected with and carry meningococcal bacteria in their nose or throat. Yet, in an average year in British Columbia, approximately 35 to 40 cases of invasive meningococcal disease are reported.[21] Therefore, meningococcus causes an estimated one case of invasive disease in approximately every 25000 to 50000 persons that are infected in a year. Unfortunately, it is not possible to predict who will develop invasive disease. Certain factors are associated with higher risk of invasive disease, such as overcrowded living conditions, exposure to tobacco smoke, recent influenza or other respiratory illness, immunosuppression or absent/nonfunctioning spleen.[8] However, most cases of invasive disease occur in previously healthy people.
Ten percent to 15% of people who develop invasive meningococcal disease die.[22,23] Up to 20% of survivors may be left with permanent disabilities, including mental retardation, loss of hearing, and amputation of extremities.[24] A successful outcome depends on early recognition of meningococcal disease, which may be difficult. The clinical appearance of early meningococcal disease often resembles a typical flu-like illness for the first few days, with headache, fever, cough, sore throat, weakness, and loss of appetite. A stiff neck and purpuric or petechial rash in conjunction with influenza symptoms can be important clues of meningococcal illness. Timely initiation of effective empiric antibiotic treatment is important; antibiotic resistance is uncommon in meningococcal isolates in British Columbia (BC Centre for Disease Control, unpublished data, 2001). Public health ensures follow-up of all recent close contacts of each case to offer antibiotics, which are highly effective at preventing infection among close contacts who, without chemoprophylaxis, have a risk of invasive disease of approximately 0.4%—about 500 times higher than the reported population incidence in British Columbia.[25] In addition to antibiotic chemoprophylaxis, BC has recently adopted NACI’s recomendation that all close contacts also be immunized with meningococcal vaccine for infections caused by a vaccine-containing serogroup.
Diagnosis and follow-up of meningococcal disease
Figure 6 outlines an algorithm for clinical and laboratory diagnosis of meningococcal disease, which also incorporates molecular diagnostic testing and public health notification.
Further information
The Statement on Recommended Use of Meningococcal Vaccines, issued by NACI on Immunization, provides a detailed, comprehensive summary of the epidemiology of meningococcal disease in Canada and options for its control and prevention, and can be viewed at www.hc-sc.gc.ca/pphbdgspsp/publicat/ccdr-rmtc/01vol27/27sup/acs6.html. Further information about meningococcal disease is available from BC Ministry of Health Services (Health File entitled Meningococcal Infection) at www.healthservices.gov.bc.ca/hlthfile/hfile23.html and from the US Centers for Disease Control and Prevention at www.cdc.gov/ncidod/dbmd/diseaseinfo/meningococcal_g.htm.
Acknowledgments
BCCDC Laboratory Services: Dr J. Isaac-Renton, Dr S. Champagne, Dr G. Stephens, Ms C. Shaw, Ms T. Rahim.
BCCDC Epidemiology Services: Dr D. Patrick, Dr M. Naus, Ms V. Yuen.
BC’s Children’s and Women’s Health Centre: Dr E. Thomas.
Competing interests
None declared.
References
1. Patrick DM, Champagne S, Taha F, et al. Distribution of Carriage of Neisseria meningitides serogroups during an outbreak intervention for serogroup C disease. Presented at: Canadian Association of Clinical Microbiology and Infectious Disease, Victoria, BC, 5–7 Nov 2001.
2. Rosenstein NE, Perkins BA, Stephens DS, et al. The changing epidemiology of meningococcal disease in the United States, 1992–1996. J Infect Dis 1999;180:1894-1901.PubMed Abstract Full Text
3. Brown S, Riley G, Jamieson F. Neisseria meningitidis with decreased susceptibility to penicillin in Ontario, Canada 1997–2000. Can Commun Dis Rep 2001;27:73-75.PubMed Citation Full Text
4. Pollard AJ, Bigham M, Shaw C, et al. Meningococcal disease in British Columbia. BC Med J 2001;43:21-27.
5. Pollard AJ, Probe G, Castell A, et al. Evaluation of a diagnostic PCR for Neisseria meningitidis and preliminary clinical experience during an outbreak in British Columbia, Canada. Arch Pathol Lab Med. In press.
6. De Wals P, De Serres G, Niyosenga T. Effectiveness of a mass immunization campaign against serogroup C meningococcal disease in Quebec. JAMA 2001;285:177-181.PubMed Abstract
7. De Wals P, Dionne M, Douville-Fradet M, et al. Impact of a mass immunization campaign against serogroup C meningococcus in the province of Quebec, Canada. Bull WHO 1996;74;407-411.PubMed Abstract
8. National Advisory Committee on Immunization. Statement on recommended use of meningococcal vaccines. 2001;27 (ACS-6):1-36. Statement on recommended use of meningococcal vaccines - CCDR Vol.27 ACS-6 (15 October 2001; retrieved 14 March 2002).
9. Ramsay ME, Andrews N, Kaczmarski EB, et al. Efficacy of meningococcal serogroup C conjugate vaccine in teenagers and toddlers in England. Lancet 2001;357:195-196.PubMed Abstract
10. MacLennan J, Obaro S, Deeks J, et al. Immunologic memory 5 years after meningococcal A/C conjugate vaccination in infancy. J Infect Dis 2001;183:97-104.PubMed Abstract Full Text
11. Salleras L, Dominguez A, Prats G, et al. Dramatic decline of serogroup C meningococcal disease incidence in Catalonia (Spain) 24 months after a mass vaccination programme of children and young people. J Epidemiol Commun Health 2001;55:283-287.PubMed Abstract
12. Committee to Advise on Tropical Medicine and Travel. Statement on meningococcal vaccination for travellers. Can Commun Dis Rep 1999;25(ACS-5).
13. US Centers for Disease Control and Prevention. Meningococcal disease and college students: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbid Mortal Wkly Rep 2000;49(RR-7):13-20.PubMed Abstract Full Text
14. MacLennan JM, Shackley F, Heath PT, et al. Safety, immunogenicity, and induction of immunologic memory by a serogroup C meninogcocccal conjugate vaccine in infants. A randomized controlled trial. JAMA 2000;283:2795-2801.PubMed Abstract
15. Richmond P, Goldblatt D, Fusco PC, et al. Safety and immunogenicity of a new Neisseria meningitidis serogroup C-tetanus toxoid conjugate vaccine in healthy adults. Vaccine 2000;18:641-646.PubMed Abstract
16. Richmond P, Borrow R, Boldblatt D, et al. Ability of 3 different meningococcal C conjugate vaccines to induce immunologic memory after a single dose in UK toddlers. J Infect Dis 2001;183:160-163.PubMed Abstract
17. Richmond P, Borrow R, Findlow J, et al. Evaluation of De-O-acetylated meningococcal C polysaccharide-tetanus toxoid conjugate vaccine in infancy: Reactogenicity, immunogenicity, immunologic priming and bactericidal activity against O-acetylated and De-O-acetylated serogroup C strains. Infect Immun 2001;69:2378-2382.PubMed Abstract Full Text
18. Hart CA, Cuevas LE. Meningococcal disease in Africa. Ann Trop Med Parasitol 1997;91:777-785.PubMed Abstract
19. Gold R, Goldschneider I, Lepow ML, et al. Carriage of Neisseria meningitidis and Neisseria lactamica in infants and children. J Infect Dis 1978:137:112-121.PubMed Abstract
20. Caugant DA, Høiby EA, Magnus P, et al. Asymptomatic carriage of Neisseria meningitidis in a randomly sampled population. J Clin Microbiol 1994;32:323-330.PubMed Abstract
21. British Columbia Centre for Disease Control. 2000 Annual Summary of Reportable Diseases. www.bccdc.org/content.php?item=33 (2000; retrieved 14 March 2002).
22. Squires SG, Pelletier L, Mungai M, et al. Invasive meningococcal disease in Canada, 1 January 1997 to 31 December 1998. Can Commun Dis Rep 2000;26:177-182.PubMed Citation Full Text
23. Whalen CM, Hockin JC, Ryan A, et al. The changing epidemiology of invasive meningococcal disease in Canada, 1985 through 1992. Emergence of a virulent clone of Neisseria meningitidis. JAMA 1995;273:390-394.PubMed Abstract
24. Erickson L, DeWals P. Complications and sequelae of meningococcal disease in Quebec, Canada, 1990–1994. Clin Infect Dis 1998;26:1159-1164.PubMed Abstract
25. Analysis of endemic meningococcal disease by serogroup and evaluation of chemoprophylaxis. J Infect Dis 1976;134:202-204. PubMed Citation
Mark Bigham, MD, FRCPC, Mary Jane Trepanier, Dipl CIS, and Simon Dobson, MD, FRCPC
Dr Bigham is a clinical assistant professor in the Department of Health Care and Epidemiology at the University of British Columbia and a physician-epidemiologist at the BC Centre for Disease Control. Ms Trepanier is a research officer at the BC Centre for Disease Control. Dr Dobson is clinical associate professor of pediatric infectious disease in the Department of Pediatrics at BC’s Children’s and Women’s Health Centre.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}