High prevalence of burnout and moral distress in orthopaedic surgeons: A Canadian cross-sectional survey study
Issue: BCMJ,
vol. 68, No. 4, May 2026,
Pages 128-134 Original Research
ABSTRACT
Background: Physician burnout is increasingly recognized as a critical issue with serious consequences for physician well-being, patient care, and the health care system. Orthopaedic surgeons are particularly susceptible to burnout due to numerous stressors surrounding work and personal obligations. The objective of this study was to determine the prevalence of, and risk factors for, burnout in Canadian orthopaedic surgeons.
Methods: Anonymous online surveys were administered to orthopaedic surgeons identified via the senior author’s university and the Canadian Orthopaedic Association’s mailing list. The survey included the Maslach Burnout Inventory, the Measure of Moral Distress for Health Care Professionals, and demographic questions. Risk factors for burnout were identified using a multivariate logistic regression model. Associations between risk factors and depersonalization and emotional exhaustion were assessed using a multivariate linear regression model.
Results: In total, 215 participants responded to the survey (response rate of 19.6%). Of those, 62.8% (135/215) screened positive for burnout. When adjusting for other factors, moral distress was identified as a risk factor for burnout (odds ratio = 1.03, 95% CI, 1.02-1.05, P < .001). Older age was negatively associated with burnout (odds ratio = 0.97, 95% CI, 0.94-0.99, P = .02). There was no association between burnout and work hours, administrative burden, sex, or level of training.
Conclusions: This is the first national study to quantify burnout and moral distress among Canadian orthopaedic surgeons using full-length validated instruments. The high prevalence of burnout, along with the strong association with moral distress, highlights the urgent need for systemic interventions targeting physician wellness.
Systemic interventions are urgently needed for orthopaedic surgeons experiencing high levels of burnout to maintain physician well-being and quality patient care.
Background
Occupational burnout is defined by a high level of emotional exhaustion, depersonalization, and a low sense of self-achievement.[1] Burnout is most commonly measured using the Maslach Burnout Inventory (MBI), a validated self-reporting instrument that measures levels of each of the three domains of burnout.[1] Physician burnout has negative consequences for the physician, their family, their patients, and the health care system as a whole. Physicians who are burned out are more likely to make medical errors and have a detached view of their patients, which leads to a lower quality of patient care.[2] Burnout negatively impacts the health care system by reducing physician productivity, increasing physician turnover, and reducing access for patients, which leads to increased costs.[3] One study estimated that in the US alone, the annual cost of physician turnover and reduced clinical hours was approximately US$4.6 billion.[4] In addition, burnout is highly comorbid with mental health issues, such as major depressive disorder, anxiety disorders, and substance use disorders. A US-based survey conducted in 2014 showed that burned-out physicians were more likely to suffer from depression and substance use disorders and were at higher risk for suicide.[5]
Physicians in the US are at a greater risk for burnout than the general population. Shanafelt and colleagues found that physicians had a 40% greater risk for occupational burnout and were 30% less satisfied with their work–life integration compared with other occupations.[6] Thus, the relatively high prevalence of physician burnout and its negative consequences on the physician, their patients, and the health care system clearly highlight the importance of preventing it.
Similarly, in Canada, burnout levels are high among practising physicians of all specialties. The 2021 Canadian Medical Association National Physician Health Survey estimated that 53% (n = 3864) of physicians in Canada experienced at least one indicator of burnout (e.g., high depersonalization, emotional exhaustion).[7] This figure was even higher for residents, with 58% of residents experiencing at least one indicator of burnout. For all respondents, there was a 22% increase in the prevalence of burnout since the previous National Physician Health Survey was conducted in 2017. Risk factors for burnout included identifying as a woman, being under the age of 54 years, having fewer years in practice, and practising in isolated or rural areas.
Other studies have identified moral distress as another important risk factor for burnout.[8] Moral distress is defined as the inability of an individual to act according to their ethical or moral beliefs due to internal and external constraints.[9] In health care, this often happens when providers recognize what they believe is the ethically correct course of action but are prevented from following it, which leads to feelings of frustration, guilt, and powerlessness.
Only a limited number of systematic reviews and meta-analyses have evaluated burnout among orthopaedic surgeons. Van Niekerk and colleagues[10] conducted an umbrella review of burnout in orthopaedic surgeons, which included eight systematic reviews and eight narrative reviews. The rates of burnout in the studies reviewed varied from 16.2% to 85.1%. Three reviews noted that residents were at greater risk for burnout than attending surgeons.[2,11,12] Compared with other specialties, orthopaedic surgeons had a similar or slightly lower risk for burnout. No subgroup analysis was performed to determine the prevalence of burnout by country. In 2020, Kollias and colleagues conducted a national survey of orthopaedic attending surgeons and trainees across Canada, using the Expanded Physician Well-Being Index; 55.4% of attending surgeons and 40.0% of trainees screened positive for distress.[13]
The objective of this study was to estimate the national prevalence of burnout in orthopaedic surgeons and identify risk factors for burnout. Although prior studies have investigated distress in Canadian orthopaedic trainees, to our knowledge, this is the first study to comprehensively assess burnout and moral distress at a national level using validated instruments. Given the increasing recognition of moral distress as a driver of burnout, particularly postpandemic, there is a need for timely data to monitor burnout levels and inform wellness strategies.
Methods
Study participants
This study was designed as a national cross-sectional study using data collected from August 2023 to October 2024. Trainees and attending-level orthopaedic surgeons associated with the senior author’s university and the Canadian Orthopaedic Association were invited to participate in the study. Anonymous online surveys were administered through Research Electronic Data Capture (REDCap).[14,15] Participants were asked to complete demographic questions, the MBI, and, optionally, the Measure of Moral Distress for Health Care Professionals (MMD-HP).[16] The MMD-HP includes an open-ended question that asks participants to identify any factors that may cause them moral distress. Participants were also asked about the number of hours worked per week, the number of hours spent on administrative tasks per week, their level of training, and their academic affiliation.
In concordance with published literature, a participant was screened positive for burnout if their emotional exhaustion score was 20 or higher or their depersonalization score was 10 or higher.[17] If a participant was screened positive for burnout, they were given a warning message at the end of the survey informing them that they were at risk for burnout. All participants were given a list of wellness resources compiled by the Canadian Medical Association, including links to crisis hotlines.[18]
Data analysis
Data were analyzed using R and SPSS.[19,20] Using the Shapiro-Wilk test, the distribution of the MMD-HP score (W = 0.915, df = 110, P < .001), the MBI depersonalization score (W = 0.946, df = 215, P < .001), and the MBI personal accomplishment score (W = 0.901, df = 215, P < .001) did not fit normal distributions. However, the distribution of the MBI emotional exhaustion score was normally distributed (W = 0.987, df = 215, P < .040). Work hours per week (W = 0.939, df = 187, P < .001) and administrative burden (W = 0.871, df = 187, P < .001) were also non-normally distributed. Therefore, the Mann-Whitney U test was used to compare MMD-HP scores, work hours per week, and administrative burden in burned-out versus nonburned-out respondents.
We fit a logistic regression model to identify risk factors and protective factors for screening positive for burnout. An unadjusted model and a model adjusted for all other variables were both analyzed. Variables used in the analysis included level of training, sex, academic affiliation, MMD-HP score, age, number of hours worked per week, and number of hours spent on administrative tasks per week. To analyze the association between emotional exhaustion and depersonalization and other variables, we fit adjusted linear regression models.
Results
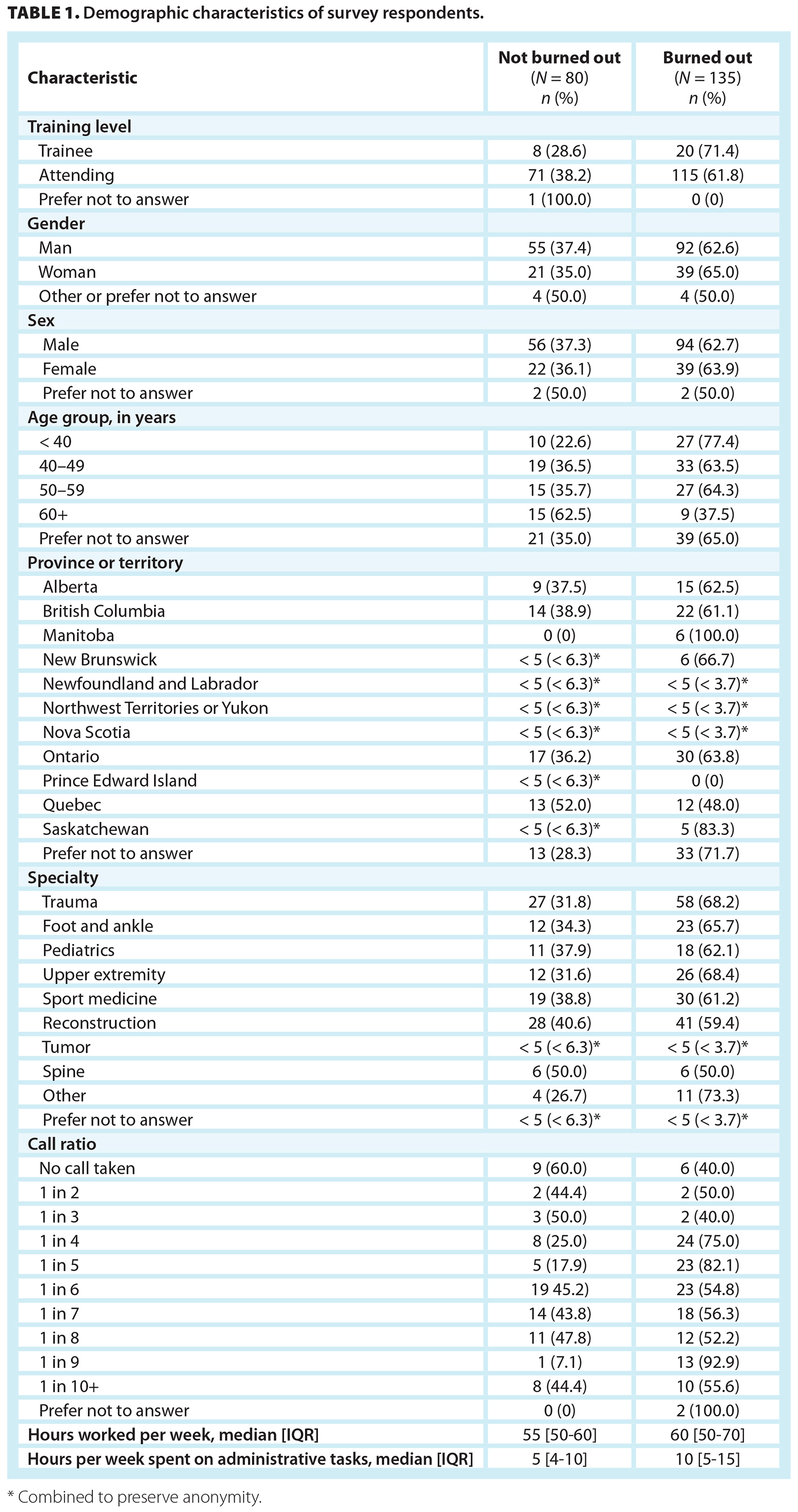
In total, 215 participants responded to the survey (19.6% response rate). Demographic characteristics of survey respondents are summarized in Table 1. Overall, 62.8% (135/215) of respondents screened positive for burnout. The study population consisted of 28 trainees (residents and fellows), 186 attending surgeons, and one participant who chose not to disclose their level of training. Of those, 61.8% (115) of attending surgeons and 71.4% (20) of trainees screened positive for burnout. The median MBI emotional exhaustion score was 28 (IQR = 18-38) for attending surgeons and 28 (IQR = 20-36) for trainees. In contrast, the median MBI depersonalization score was 9 (IQR = 4-15) for attending surgeons and 11 (IQR 7-19) for trainees.
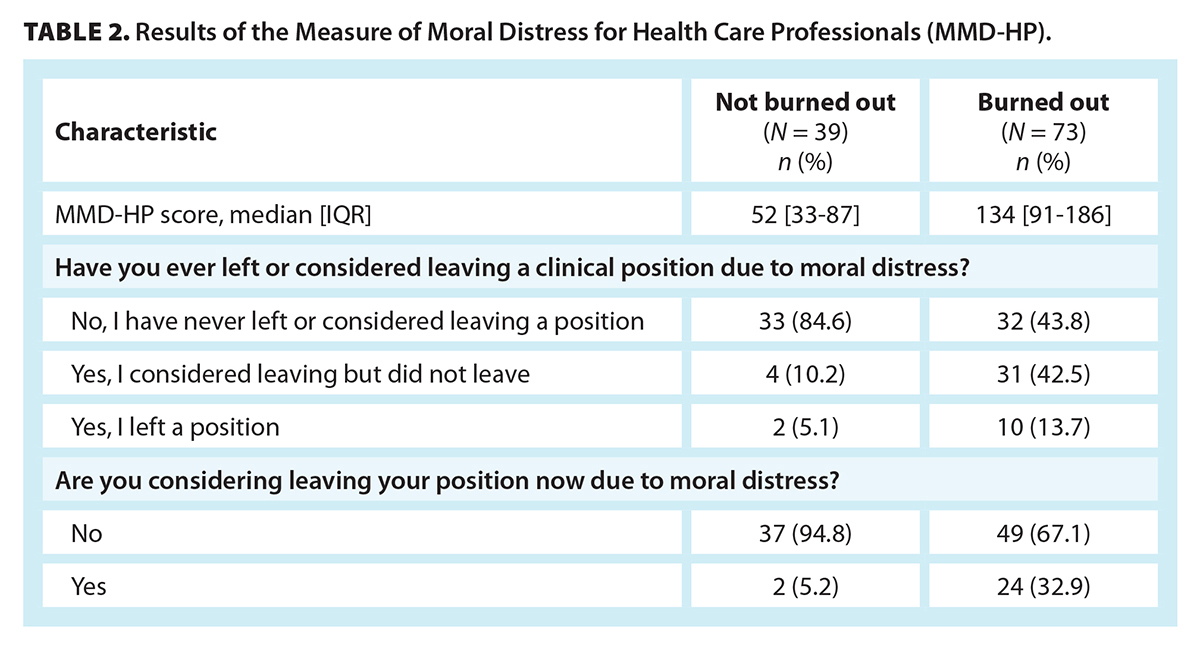
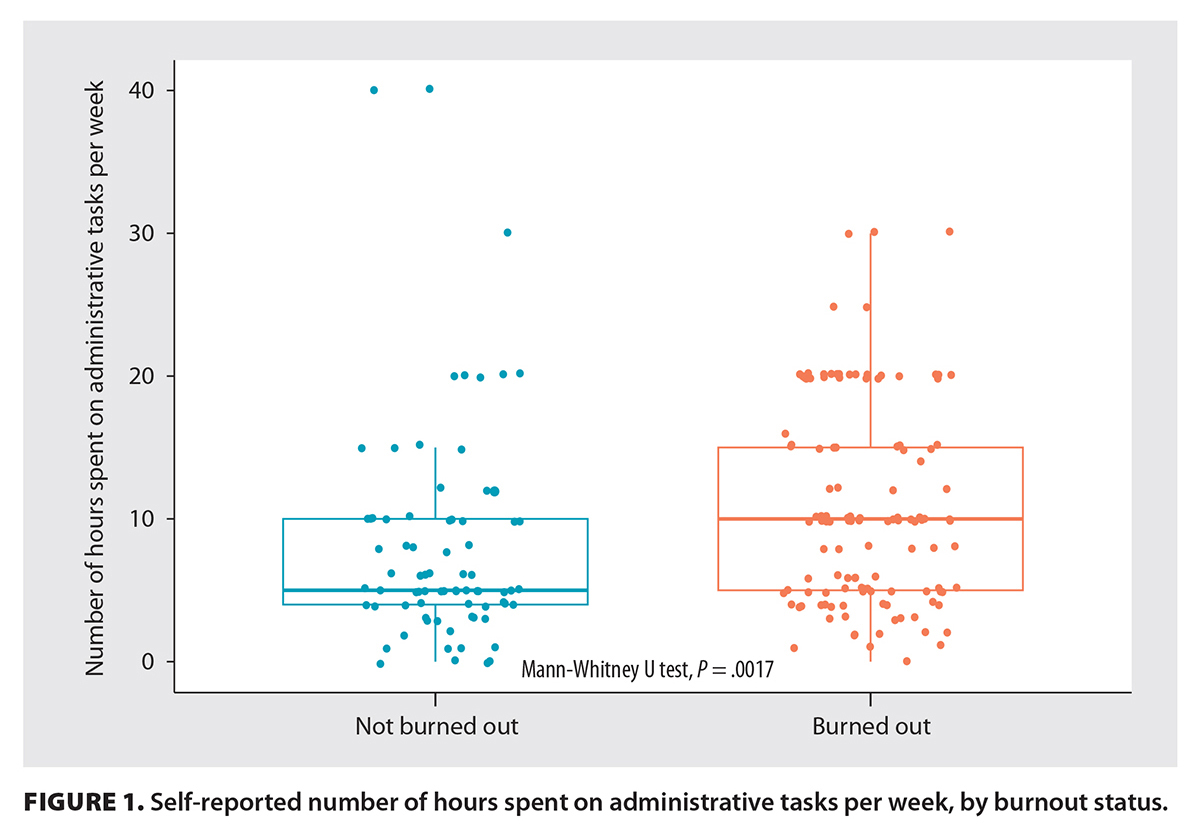
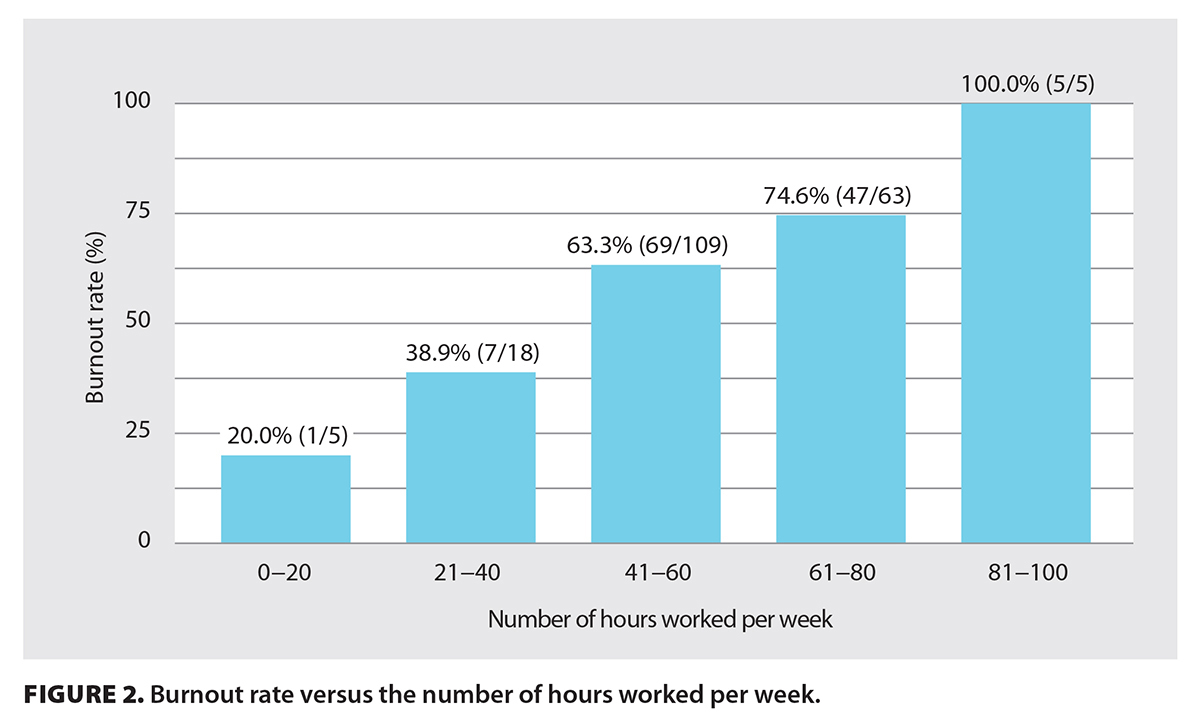
The median MMD-HP score was 52 (IQR = 33-87) for nonburned-out physicians and 134 (IQR = 91-186) for burned-out physicians (P < .001) [Table 2]. Among burned-out physicians, 32.9% (24/73) reported that they were considering leaving their position due to moral distress [Table 2]. Burned-out physicians spent more hours per week on administrative tasks than did nonburned-out physicians (P = .002) [Figure 1]. Burned-out physicians also spent more time at work than did nonburned-out physicians (P < .001); 100% of surgeons who worked 81 to 100 hours per week screened positive for burnout [Figure 2].
 |
 |
An adjusted logistic regression model identified the MMD-HP score as positively associated with burnout (odds ratio = 1.03, 95% CI, 1.02-1.05, P < .001). Older age was negatively associated with burnout (odds ratio = 0.97, 95% CI, 0.94-0.99, P = .02). In the unadjusted model, academic affiliation was negatively associated with burnout. Additionally, hours worked per week and time spent on administrative tasks per week were positively associated with burnout. However, these associations were not significant when adjusting for other factors. Neither sex nor level of training was significant in either model.
Linear regression adjusted for other factors showed a positive association between the MMD-HP score and the MBI emotional exhaustion score (β = 0.09, 95% CI, 0.05-0.12, P < .001). Age was negatively associated with emotional exhaustion (β = −0.35, 95% CI, −0.64 to −0.07, P < .018). No other factors were significantly associated with emotional exhaustion.
With respect to associations with depersonalization, the MMD-HP score (β = 0.05, 95% CI, 0.04-0.07, P < .001) and male sex (β = 3.5, 95% CI, 0.56-6.50, P = .023) were positively associated with depersonalization. Age (β = −0.18, 95% CI, −0.33 to −0.04, P < .014) and academic affiliation (β = −3.39, 95% CI, −0.17 to 0.02, P = .031) were negatively associated with depersonalization. No other factors were significantly associated with depersonalization.
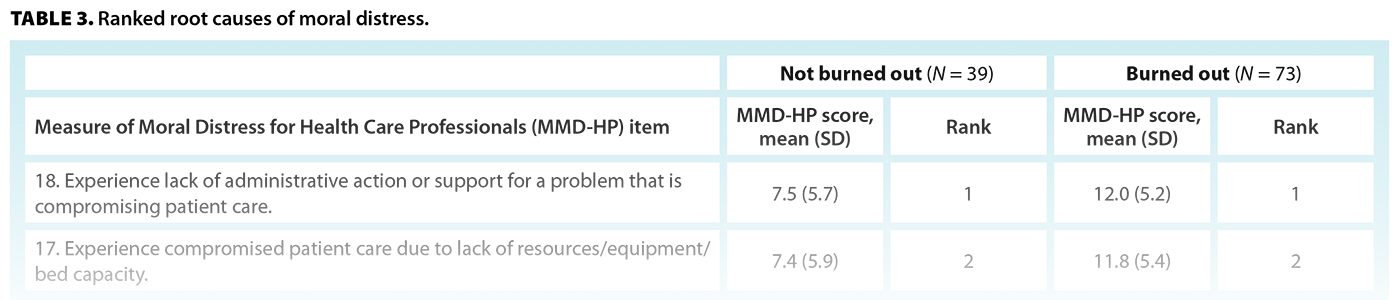
The top three root causes of moral distress were experiencing a lack of administrative action or support for a problem that was compromising patient care; experiencing compromised patient care due to a lack of resources, equipment, and/or bed capacity; and being unable to provide optimal care due to pressures from administrators or insurers to reduce costs [Table 3]. Other causes of moral distress reported in open-ended answers included long surgical wait times, conflict and bullying in the workplace, frustration with leadership, and dishonest behavior of colleagues.
Discussion
Moral distress and burnout
In this national cross-sectional study, the prevalence of burnout among orthopaedic surgeons who responded to the survey was 62.8%. Moral distress was positively associated with burnout, emotional exhaustion, and depersonalization. These results suggest that the prevalence of burnout in Canadian orthopaedic surgeons is alarmingly high, and moral distress may play a role in precipitating it.
The reported prevalence of burnout in orthopaedic surgeons varies significantly across studies. An umbrella review of 26 studies reported a prevalence of burnout ranging from 16.2% to 85.1%.[10] This substantial heterogeneity in results may be explained partially by the variety of tools used to measure burnout, the different definitions of burnout used, and the spatial and temporal variability of study populations. The gold standard instrument for screening for burnout is the MBI; however, due to the lengthy nature of the instrument, it is not used by all researchers. For instance, an abbreviated two-item version of the MBI and other tools for measuring distress, such as the Expanded Physician Well-Being Index, have been used to increase response rates.[13,21] Consequently, researchers use different definitions and cutoffs for burnout, which introduces further heterogeneity in the prevalence of burnout reported in different studies.
In our study, younger age was a risk factor for burnout. This is consistent with the results of previous studies.[2,7] However, our findings are not fully concordant with previous research, which cites trainee status, female sex, lack of academic affiliation, increased hours worked per week, and increased administrative burden as risk factors.[22-25] In our study, there was a strong trend between hours worked per week and prevalence of burnout. This trend, in addition to the narrow confidence interval and near-significant P value, suggests that although hours worked may not be a statistically significant risk factor, it may still have clinical significance.
Our study suggests there is a strong association between moral distress and burnout, which is concordant with the limited findings from previous research. Notably, in our study, 56.2% of surveyed orthopaedic surgeons who screened positive for burnout had either left or considered leaving due to moral distress. This suggests that moral distress may play a role in further exacerbating the existing physician shortage in Canada. Likewise, moral distress has also been found to be associated with higher levels of burnout in critical care providers and internists.[8,26] A survey of 479 physicians during the COVID-19 pandemic also found a correlation between moral distress and burnout; however, the pandemic may have played a role in precipitating both burnout and moral distress.[27] The root causes of moral distress include many scenarios that can be stressful to physicians; this makes it difficult to discern whether there is a causal link between moral distress and burnout. There is a complex interplay between moral distress, negative work–home interactions, and other risk factors, which may all contribute to burnout.[28] Overall, saying that moral distress is a cause of burnout is an oversimplification and discounts other variables at play.
Interventions to address burnout
Given the high prevalence of burnout in orthopaedic surgeons and other physicians, strategies to address burnout are of utmost importance for physician well-being and to improve quality of care for patients. However, published research on this subject is limited. Previous researchers have described a top-down approach to promoting surgeon well-being. It prioritizes interventions at the institutional level, followed by seeking professional support services; individual practices are the final and least-emphasized layer of intervention.[29]
Institutional-level interventions target workload, workflow, autonomy, and reduction in administrative burden. They are generally more efficacious than individual-level interventions that address burnout.[30] For instance, efforts to streamline electronic health record systems, including incorporation of the use of medical scribes and electronic health record training, have shown benefits in reducing administrative burden and, subsequently, physician burnout.[31] However, modifications to electronic health record systems that focus on data-entry automation or revision of electronic health record forms and workflow were not consistently associated with a reduction of burnout.[31] Additionally, there has been increasing interest in the use of ambient artificial intelligence (AI) scribes to aid in medical documentation during clinical encounters. These AI scribes listen in on clinician–patient interactions and use large language models to automate documentation of clinic notes. A large RCT of two AI scribe applications showed improvements in physician burnout and task load and reduced time spent documenting compared with manual documentation.[32] A multicentre quality improvement study also showed that the use of ambient AI scribe technology had a positive effect on burnout and reduced administrative burden.[33]
Several RCTs have shown that peer support discussion groups are also effective in reducing burnout and depressive symptoms and improving job satisfaction in practising physicians.[34,35] In this institutional-level intervention, physicians are supported by having employer-provided protected time to participate in facilitated group discussions that promote well-being and distress management. This suggests that self-facilitated peer support group meetings are an effective low-cost strategy to improve physician well-being and reduce burnout.
Other interventions have focused on the use of professional assistance in developing self-directed reliance and emotional regulation strategies. Professional coaching is an example of such an intervention; it involves one-on-one coaching provided by trained coaches who support physicians in improving self-awareness, motivation, and self-efficacy.[36] An RCT of 79 internal medicine attending physicians found that one-on-one coaching was associated with a long-lasting 13.4% absolute reduction in burnout, whereas burnout increased by 11.1% in a control group of physicians.[36] Other studies have explored the establishment of wellness teams consisting of counseling and psychiatric support services. Regular meetings with trained counselors have shown potential in reducing burnout in medical residents.[37]
Individual-level interventions are the least effective in managing burnout but still play an important role when used in addition to institutional-level interventions. An RCT found that mindfulness-based meditation was effective in reducing burnout, stress, and anxiety in orthopaedic surgery residents at a single institution.[38] Other individual interventions include stress management workshops and exercise programs.[39,40] Weight and colleagues explored the effects of a 12-week team-based incentivized exercise program on quality of life and burnout in a cohort of 1060 residents and fellows.[39] Fewer regular exercise program participants screened positive for burnout compared with nonparticipants, although this result was not statistically significant.[38] Overall, individual-level interventions should be used as an adjunct to institutional-level interventions in treating burnout.
Study limitations
The primary limitation of our study was our response rate of 19.6%, which may have led to nonresponse bias. It is possible that surgeons who were experiencing higher levels of burnout were more compelled to respond due to personal relevance or, conversely, were less likely to respond due to emotional exhaustion. Despite the modest response rate, it is comparable to other physician health surveys, including the 2021 Canadian Medical Association National Physician Health Survey (response rate of ~18%).[7,13] Second, our study was cross-sectional in nature and did not explore changes in burnout or moral distress over time. Last, while interventions to address burnout are important, further research is needed to investigate the efficacy of specific interventions within the context of orthopaedic surgery. Given the association between moral distress and burnout, interventions aimed at addressing moral distress may be effective in concurrently reducing moral distress and burnout. Interventions should follow a top-down approach, which should include institutional-level interventions in addition to individual-level interventions.
Our study also had several strengths. This was the first national study to estimate the prevalence of and identify risk factors for burnout in orthopaedic surgeons in Canada. In addition, the use of the full-length MBI, a validated instrument and the widely accepted gold standard for measuring burnout, enhanced the validity of our findings. We also investigated a wide range of potential risk and protective factors for burnout, thereby providing a holistic view of the survey respondents.
Conclusions
Nearly two out of three surveyed orthopaedic surgeons were screened as burned out. Moral distress and younger age were positively associated with burnout. Addressing burnout is important for physician well-being and providing quality patient care.
Acknowledgments
We would like to graciously thank the Canadian Orthopaedic Association for its support in distributing the surveys in our study.
Ethics approval and consent to participate
Research ethics approval was obtained from the University of British Columbia Children’s and Women’s Research Ethics Board (H22-03652).
Competing interests
None declared.
This article has been peer reviewed.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
References
1. Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav 1981;2:99-113. https://doi.org/10.1002/job.4030020205.
2. Hui RWH, Leung KC, Ge S, et al. Burnout in orthopaedic surgeons: A systematic review. J Clin Orthop Trauma 2019;10:S47-S52. https://doi.org/10.1016/j.jcot.2019.01.028.
3. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: Contributors, consequences and solutions. J Intern Med 2018;283:516-529. https://doi.org/10.1111/joim.12752.
4. Han S, Shanafelt TD, Sinsky CA, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med 2019;170:784-790. https://doi.org/10.7326/M18-1422.
5. Lacy BE, Chan JL. Physician burnout: The hidden health care crisis. Clin Gastroenterol Hepatol 2018;16:311-317. https://doi.org/10.1016/j.cgh.2017.06.043.
6. Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc 2015;90:1600-1613. https://doi.org/10.1016/j.mayocp.2015.08.023.
7. Canadian Medical Association. CMA 2021 national physician health survey. 24 August 2022. Accessed 17 February 2026. https://digitallibrary.cma.ca/link/digitallibrary17.
8. Fumis RRL, Junqueira Amarante GA, de Fátima Nascimento A, Vieira Junior JM. Moral distress and its contribution to the development of burnout syndrome among critical care providers. Ann Intensive Care 2017;7:71. https://doi.org/10.1186/s13613-017-0293-2.
9. Canadian Medical Association. COVID-19 and moral distress. March 2020. Accessed 17 February 2026. https://digitallibrary.cma.ca/link/digitallibrary54.
10. van Niekerk M, Tileston K, Bouchard M, et al. A comprehensive umbrella review for understanding burnout in orthopaedic surgery. J Pediatr Soc North Am 2024;5:619. https://doi.org/10.55275/JPOSNA-2023-619.
11. Arora M, Diwan AD, Harris IA. Burnout in orthopaedic surgeons: A review. ANZ J Surg 2013;83:512-515. https://doi.org/10.1111/ans.12292.
12. Pulcrano M, Evans SRT, Sosin M. Quality of life and burnout rates across surgical specialties: A systematic review. JAMA Surg 2016;151:970-978. https://doi.org/10.1001/jamasurg.2016.1647.
13. Kollias CM, Okoro T, Tufescu TV, Wadey V. Distress in orthopedic trainees and attending surgeons: A Canadian national survey. Can J Surg 2020;63:E190-E195. https://doi.org/10.1503/cjs.004319.
14. Harris PA, Taylor R, Thielke R, et al. Research Electronic Data Capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-381. https://doi.org/10.1016/j.jbi.2008.08.010.
15. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208.
16. Epstein EG, Whitehead PB, Prompahakul C, et al. Enhancing understanding of moral distress: The measure of moral distress for health care professionals. AJOB Empir Bioeth 2019;10:113-124. https://doi.org/10.1080/23294515.2019.1586008.
17. Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: A systematic review. JAMA 2018;320:1131-1150. https://doi.org/10.1001/jama.2018.12777.
18. Canadian Medical Association. Physician wellness support services. Accessed 28 December 2024. www.cma.ca/physician-wellness-support-services.
19. RStudio Team. RStudio: Integrated development for R. Boston, MA: RStudio, PBC; 2020. Accessed 23 October 2024. www.rstudio.com/.
20. IBM. IBM SPSS Statistics. Accessed 15 March 2026. www.ibm.com/products/spss-statistics.
21. Shanafelt TD, West CP, Sinsky C, et al. Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2020. Mayo Clin Proc 2022;97:491-506. https://doi.org/10.1016/j.mayocp.2021.11.021.
22. Sargent MC, Sotile W, Sotile MO, et al. Stress and coping among orthopaedic surgery residents and faculty. J Bone Joint Surg Am 2004;86:1579-1586. https://doi.org/10.2106/00004623-200407000-00032.
23. Saleh KJ, Quick JC, Sime WE, et al. Recognizing and preventing burnout among orthopaedic leaders. Clin Orthop Relat Res 2009;467:558-565. https://doi.org/10.1007/s11999-008-0622-8.
24. Sargent MC, Sotile W, Sotile MO, et al. Managing stress in the orthopaedic family: Avoiding burnout, achieving resilience. J Bone Joint Surg Am 2011;93:e40. https://doi.org/10.2106/JBJS.J.01252.
25. Mir H, Downes K, Chen AF, et al. Physician wellness in orthopaedic surgery: A multinational survey study. Bone Jt Open 2021;2:932-939. https://doi.org/10.1302/2633-1462.211.BJO-2021-0153.
26. Sajjadi S, Norena M, Wong H, Dodek P. Moral distress and burnout in internal medicine residents. Can Med Educ J 2017;8:e36-e43.
27. Powell CAJ, Butler JP. The role of moral distress on physician burnout during COVID-19. Int J Environ Res Public Health 2022;19:6066. https://doi.org/10.3390/ijerph19106066.
28. Kok N, Van Gurp J, van der Hoeven JG, et al. Complex interplay between moral distress and other risk factors of burnout in ICU professionals: Findings from a cross-sectional survey study. BMJ Qual Saf 2023;32:225-234. https://doi.org/10.1136/bmjqs-2020-012239.
29. Jennings JM, Gold PA, Nellans K, Boraiah S. Orthopaedic surgeons have a high prevalence of burnout, depression, and suicide: Review of factors which contribute or reduce further harm. J Am Acad Orthop Surg 2022;30:e528-e535. https://doi.org/10.5435/JAAOS-D-21-00299.
30. Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern Med 2017;177:195-205. https://doi.org/10.1001/jamainternmed.2016.7674.
31. Kang C, Sarkar IN. Interventions to reduce electronic health record-related burnout: A systematic review. Appl Clin Inform 2024;15:10-25. https://doi.org/10.1055/a-2203-3787.
32. Lukac PJ, Turner W, Vangala S, et al. A randomized-clinical trial of two ambient artificial intelligence scribes: Measuring documentation efficiency and physician burnout. medRxiv 2025:25331333. https://doi.org/10.1101/2025.07.10.25331333.
33. Olson KD, Meeker D, Troup M, et al. Use of ambient AI scribes to reduce administrative burden and professional burnout. JAMA Netw Open 2025;8:e2534976. https://doi.org/10.1001/jamanetworkopen.2025.34976.
34. West CP, Dyrbye LN, Satele DV, Shanafelt TD. Colleagues Meeting to Promote and Sustain Satisfaction (COMPASS) groups for physician well-being: A randomized clinical trial. Mayo Clin Proc 2021;96:2606-2614. https://doi.org/10.1016/j.mayocp.2021.02.028.
35. West CP, Dyrbye LN, Rabatin JT, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: A randomized clinical trial. JAMA Intern Med 2014;174:527-533. https://doi.org/10.1001/jamainternmed.2013.14387.
36. Dyrbye LN, Shanafelt TD, Gill PR, et al. Effect of a professional coaching intervention on the well-being and distress of physicians: A pilot randomized clinical trial. JAMA Intern Med 2019;179:1406-1414. https://doi.org/10.1001/jamainternmed.2019.2425.
37. Broxterman J, Jobe A, Altenhofen D, Eck L. Promoting resident well-being through programmatic scheduled wellness consultation. J Gen Intern Med 2019;34:659-661. https://doi.org/10.1007/s11606-019-04877-z.
38. Boden LM, Rodriguez C, Kelly JD, et al. Mindfulness applications: Can they serve as a stress, anxiety, and burnout reduction tool in orthopaedic surgery training? A randomized control trial. JBJS Open Access 2023;8:e22.00114. https://doi.org/10.2106/JBJS.OA.22.00114.
39. Weight CJ, Sellon JL, Lessard-Anderson CR, et al. Physical activity, quality of life, and burnout among physician trainees: The effect of a team-based, incentivized exercise program. Mayo Clin Proc 2013;88:1435-1442. https://doi.org/10.1016/j.mayocp.2013.09.010.
40. Margalit APA, Glick SM, Benbassat J, et al. Promoting a biopsychosocial orientation in family practice: Effect of two teaching programs on the knowledge and attitudes of practising primary care physicians. Med Teach 2005;27:613-618. https://doi.org/10.1080/01421590500097091.
Mr Leong is a medical student in the Faculty of Medicine, University of British Columbia. Dr Chhina is a research associate in the Department of Orthopaedics, UBC. Dr Cooper is a clinical professor in the Department of Orthopaedics, UBC, and the head of the Department of Orthopaedics, BC Children’s Hospital.
Corresponding author: Dr Anthony Cooper, externalfixators@cw.bc.ca.
