Original Research
Eliminating the routine use of examination table paper in outpatient oncology clinics
Issue: BCMJ,
vol. 66 , No. 6 , July August 2024 ,
Pages 204-209 Clinical Articles Original Research
ABSTRACT
Background: Health care systems contribute significantly to greenhouse gas emissions. One source of these emissions is single-use products. Examination table paper does not confer protection against microbial contamination and thus can be omitted while following infection control standards. The objective is to eliminate the routine use of examination table paper in outpatient oncology clinics at BC Cancer.
Methods: A quality improvement approach was used. Examination tables continued to be disinfected using wipes between patients, but table paper was not used. Plan-do-study-act cycles were performed at four regional cancer centres.
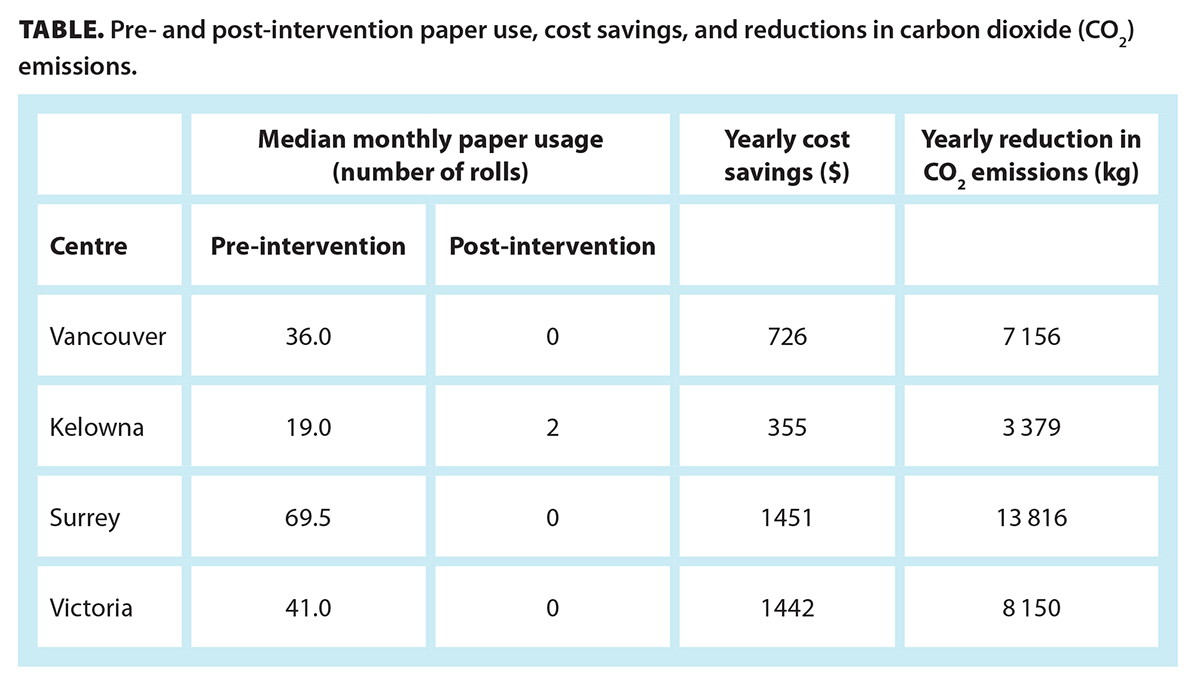
Results: Pre-intervention, the cancer centres used 19 to 69 rolls of paper monthly. Post-intervention, usage declined to 0 to 2 rolls monthly. This was associated with annual cost savings of $3974 and a reduction of 32 501 kg of carbon dioxide emissions.
Conclusions: The use of examination table paper can be eliminated in outpatient clinics, resulting in both cost savings and a reduction in carbon dioxide emissions.
Cost savings and greenhouse gas emission reductions can be achieved by eliminating the use of examination table paper in clinics.
Background
Climate change is a continuously growing threat, and the resulting environmental and societal instability significantly impacts not only human health but also the health care sector as a whole. As the climate continues to destabilize, extreme weather events disrupt services and infrastructure, superbugs increase in prevalence, and food security is threatened.[1] In their current state, the health care sector’s operations exacerbate the climate crisis by generating vast waste and engaging in carbon-intensive practices, which creates a detrimental feedback loop.[2]
The health care sector contributes approximately 5% of the world’s greenhouse gas emissions, which emphasizes the pivotal role that implementing low-carbon, low-waste health care practices plays in mitigating climate change. Emissions from providing health care are grouped into three categories, as defined by global greenhouse gas accounting standards. Scope 1 includes direct facility emissions, such as those from fossil fuel heating systems and anesthetic gases. Scope 2 includes indirect emissions from energy purchased—typically electricity. Scope 3 includes emissions attributed to the global health care supply chain, which represent 60% to 80% of health care–related emissions. This includes the production, transport, and disposal of goods such as pharmaceuticals, food, medical devices, hospital equipment, and instruments.[3-5]
Covering clinical examination tables with thin white paper (referred to as table paper) is an example of a wasteful practice involving a single-use item. This practice has become entrenched in outpatient clinical care. Typically, a roll of paper is attached to the table, and the paper is changed after every patient. Although the paper may be recyclable in some jurisdictions, most commonly it is thrown into standard garbage due to fears of microbial contamination. Its presence conveys the appearance of a sterile medical environment. However, it adds no protection against surface-borne bacteria or viruses.[6,7]
While ample data indicate that surfaces such as examination tables can harbor microbes,[8-10] infection control guidance recommends cleaning surfaces with hospital-grade disinfectants between patients. The use of a barrier, such as table paper, does not replace the need for cleaning.[11-13] Elimination of table paper has been subject to a number of sustainable quality improvement initiatives.[14-16] To our knowledge, this had not been implemented in large ambulatory care centres or in centres that routinely care for immunocompromised patients.
In the past, examination tables in the ambulatory clinics at BC Cancer were cleaned with disinfectant wipes between patients, followed by a change of the table paper. Several clinicians noted that this practice resulted in unnecessary waste and effort. The concern was escalated to the BC Cancer Planetary Health Unit, a clinician-led initiative focused on promoting low-carbon, low-waste, and high-quality sustainable health care practices. Under the leadership of the BC Cancer Planetary Health Unit, a sustainable quality improvement project was developed to eliminate the routine use of table paper in outpatient oncology clinics.
Methods
Context
British Columbia has a population of 5 million people, and more than 30 000 new cancer diagnoses are made in the province yearly. BC Cancer is a population-based provincial care system that provides oncology services to the residents of BC. The system consists of six regional cancer centres. The largest facility, BC Cancer – Vancouver, has 80 beds that are used for ambulatory care visits.
A multidisciplinary team comprising clinical experts, primarily from the first and largest study site (the Vancouver centre); operations leaders at the provincial and regional centres; and ambulatory clinic managers adopted a quality improvement approach to eliminating the routine use of table paper in outpatient oncology clinics. This involved problem identification, setting targets, measuring success, testing changes using plan-do-study-act cycles, and eventually standardizing the change. Local and infection prevention and control services supported this initiative.
Study design
A literature review and workflow mapping were conducted. Redundancy in the existing process was identified: exam table paper was used after the table was cleaned with disinfectant wipes.
A before-and-after study design was employed. To address the impact of reduced in-person clinic visits due to COVID-19, we expanded the pre-intervention period. Pre-intervention data extended from 1 January 2019 to 30 June 2022; post-intervention data extended from 1 July 2022 to 30 June 2023. Two regional centres were excluded: one did not use exam table paper; the other had not implemented the change in procedure during the evaluation period.
 Interventions
Interventions
The first plan-do-study-act cycle occurred at BC Cancer – Vancouver, and then was replicated at three other centres: Kelowna, Victoria, and Surrey. The project team planned the change in procedure with cleaning staff. A new standard workflow was implemented: table paper was removed, and staff were required to wipe the exam table after each patient appointment. Table disinfection rates and practices were not deliberately modified as part of the intervention. Information posters explaining the intervention and rationale for its use were placed in examination rooms [Figure 1]. The posters included an email address for patients and providers to provide feedback about the intervention and a QR code that linked to infection control documents for patients or staff who desired more information. For patient comfort, table paper was still available upon patient or health care provider request.
Assumptions
BC Cancer, a program of the Provincial Health Services Authority, procures medical supplies through Provincial Health Services Authority centralized procurement. In this study, monthly quantities of rolls of table paper purchased served as a proxy for usage. A run chart that displayed the data was used to identify trends and shifts in usage.
Due to limitations in the available data, the amount of carbon dioxide (CO2) emissions saved by eliminating the use of table paper was calculated based on the following assumptions:
- The emission factor of table paper is equivalent to that of office paper. This assumption was based on aligning paper types with known emission factors. The 2020 B.C. Best Practices Methodology for Quantifying Greenhouse Gas Emissions, published by the BC Ministry of Environment and Climate Change Strategy, provides established emission factors for office paper. While exam table paper might have distinct properties, using the office paper emission factor offered a pragmatic approach to determining approximate emissions.[16]
- Exam table paper is a 0% post-consumer recycled product. Given that manufacturers often market recycled paper as a selling point and charge a higher price for such products, it is reasonable to conclude that a lower-priced product likely does not have any recycled content unless specified.
Statistical analysis
Microsoft Excel was used to generate run charts. To identify trends and deviations in the data, we computed the median value of monthly purchases of table paper and incorporated a median line into the chart. Statistical rules for detecting special cases encompassed a run consisting of seven or more consecutive points on either side of the median line, a trend consisting of seven or more consecutive points moving upward or downward, too few or too many runs, or astronomical data points.
To quantify CO2 emissions, we first calculated the total number of table paper rolls saved from July 2022 to June 2023 and estimated the equivalence to the number of 500-sheet 11″ × 17″ office paper packages. Subsequently, we determined the cumulative weight of the office paper packages based on the manufacturers’ information. Finally, we used the 2020 B.C. Best Practices Methodology for Quantifying Greenhouse Gas Emissions for office paper to compute the overall emission savings.[16]
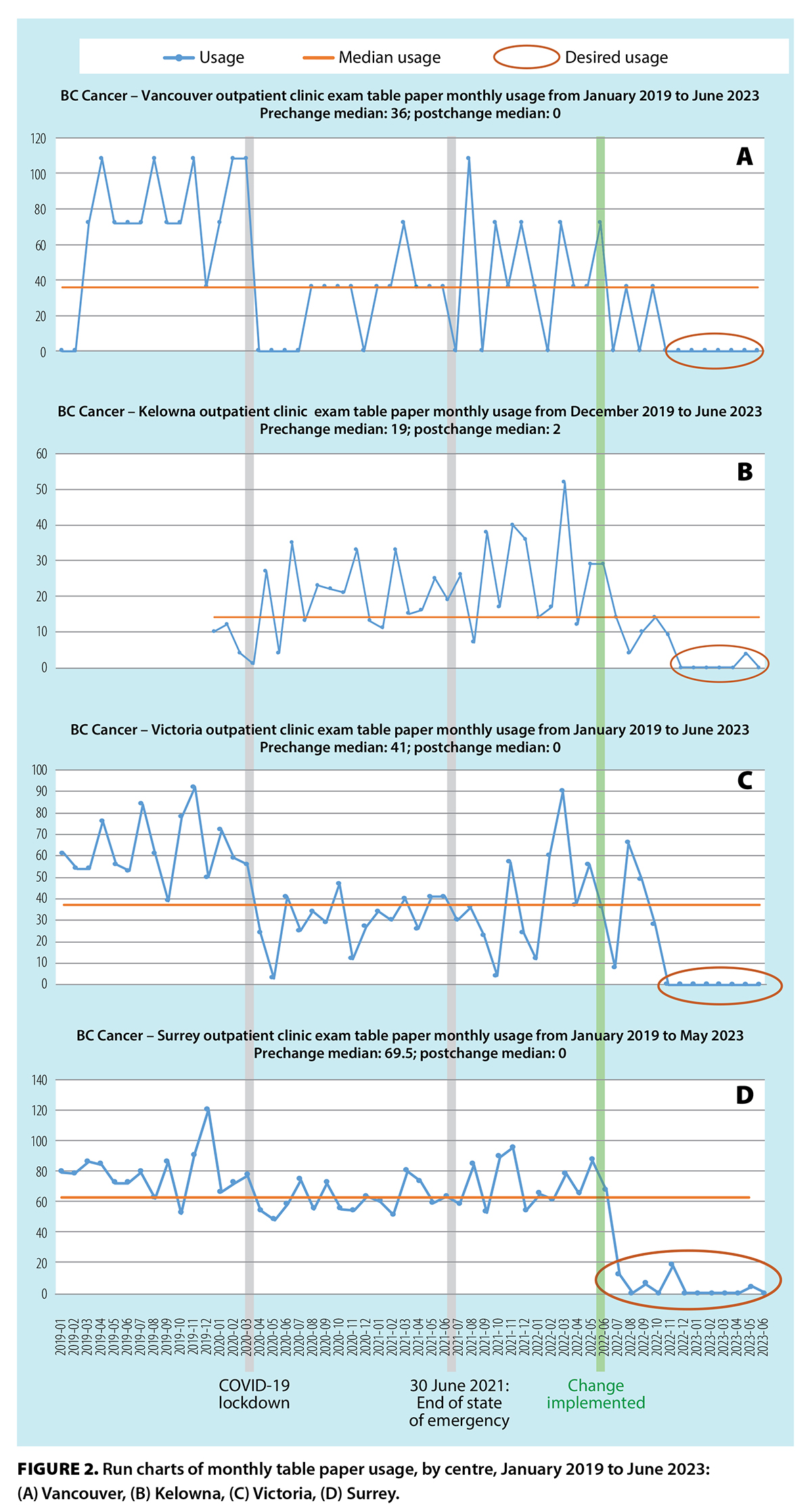
The Vancouver centre commenced eliminating the use of table paper in June 2022. Continuous monitoring and feedback from frontline staff revealed no major issues; thus, the change was implemented in the other three centres by December 2022.
At the Vancouver centre pre-intervention, 36 rolls of table paper were used monthly; post- intervention, no table paper was used. This translated to a savings of $726 and a reduction of 7156 kg of CO2 emissions per year. Similar observations were noted post-intervention at the other three centres [Table]. No table paper purchases were recorded for the Vancouver and Victoria centres after November 2022, indicating a sustained change after the intervention period.
 Results
Results
The run charts exhibited desired shifts in the use of table paper in all four centres [Figure 2]. The significant reduction in paper usage from April 2020 to June 2021 was due to the decrease in ambulatory visits during the COVID-19 lockdown.
No direct feedback about the intervention was received from patients; however, feedback from providers was largely positive. Some providers remarked that older exam tables had become sticky with exposure to chemical-grade disinfectant wipes over time. Table paper continued to be used on those tables until they could be replaced.
Discussion
Our study demonstrated the feasibility of implementing a large-scale, sustainable, quality improvement initiative, which achieved both cost savings and a reduction in CO2 emissions. The intervention was largely successful, with nearly zero usage of table paper post-intervention. The total of 32 501 kg CO2 emissions avoided though this initiative is equivalent to driving 134 087 km in an average gasoline-powered passenger vehicle.[18] Although a number of health care sustainability teams have initiated similar projects, to our knowledge this is one of the largest such initiatives and the only one to include a substantial population of immunocompromised patients.
The study had additional benefits for our centres. Although not measured in this study, we observed decreased workload for care aides, because they were no longer faced with the extra task of changing the table paper. A similar small project in a university health centre found that cleaning time was reduced by more than half when table paper was omitted.[15]
The dramatic and sustained decrease in table paper purchasing demonstrates the cultural shift that occurred with the intervention. Although table paper was still available for patients and clinicians to use, it was easily recognized that it ultimately provided no value in our clinics. Although we did not receive any direct feedback from patients, the low usage of paper after the intervention suggests that they were supportive of the intervention. Although there was some initial concern from clinics about cases where bodily fluids could be released during physical examinations, absorptive pads and washable surgical cotton cloths proved to be more suitable alternatives to table paper. The elimination of table paper and the associated posters also provided a visual reminder of work being done by the BC Cancer Planetary Health Unit. The availability of the contact information on the posters allowed clinicians to contact the project team, provide feedback, and suggest other initiatives.
Study limitations
We did not measure any balancing metrics because the standard practice at our facilities was to wipe tables in addition to using table paper. Table disinfection rates were not measured as part of the intervention. However, we recognize that in many ambulatory settings, table paper is used as a “marker” of whether the table has been used during a clinical encounter. Thus, it is possible that wipe usage increased. Because of the variety of disinfectant products used and multiple uses of the wipes, it was not possible to easily capture these data using procurement data. We also were not able to accurately measure whether the usage of other products such as disposable absorptive pads or bedsheets increased post-intervention.
We recognize that the practice of wiping tables and other medical equipment with single-use products between patients in the ambulatory setting, while compliant with infection control standards, creates large volumes of waste. In addition, the regular use of disinfectant wipes may quickly degrade the table surface, which may result in replacement of the equipment sooner than usual. Our project team hopes to explore alternatives to this practice to help reduce this burden. For example, the use of ultraviolet light has been shown to reduce microbial contamination on medical equipment without the need for manual disinfection.[19] Biodegradable wipes and wipes with recycled content are also becoming increasingly available on the market.
In addition, potential bias may have been introduced by the adoption of virtual clinic practices. The COVID-19 pandemic has had a substantial impact on health care practices, including outpatient visit patterns. The decrease and subsequent increase in in-person outpatient visits due to lockdowns and subsequent changes in health-seeking behaviors could have confounded the observed trends in the usage of exam table paper. However, the use of virtual clinics aligns with the larger project objectives in that CO2 emissions are reduced due to a decrease in the use of table paper and the use of transportation to attend clinics.
Finally, in calculating the reduction in CO2 emissions, we had to make several assumptions. Without readily available information on the recycled content of exam table paper, it is reasonable to assume that it is 0% post-consumer recycled, but this may result in an overestimation of the environmental benefits of eliminating its usage. However, this approach aligns with common practice in quality improvement outcome assessment when precise data are lacking.
The exclusion of two regional centres from the study highlights potential improvement opportunities. One centre, the newest in the system, had never used exam table paper. This highlights the importance of taking a more proactive approach to waste management in health care. The other centre delayed the change in using exam table paper because additional time was required to map the new operational flow in the clinics. Nevertheless, these challenges have been managed, and the change is expected to take place in the next 6 months.
Conclusions
We hope that our project will inspire other centres to initiate the change from using paper on examination tables. The recognition of this wasteful practice by a small group of clinicians ultimately catalyzed a change across hundreds of clinic rooms. There is much more work to do to decarbonize the health care system. A collective and collaborative global effort is required to invoke the necessary shifts in norms, policies, and investments.[2] Various credible examples of mitigation tactics have been used worldwide, ranging from low-carbon or renewable energy strategies to changes in the use of single-use items in clinical practice.[20] The cumulative effects of individual and collective efforts are vital to relieving the consequential impacts of climate change.
Competing interests
None declared.
Acknowledgments
The authors would like to thank the entire BC Cancer Planetary Health Unit steering committee for their support in planning and disseminating this project. The authors invite any clinicians in British Columbia who are hoping to undertake this intervention in their practice to contact them for advice and support.
This article has been peer reviewed.
 |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. |
References
1. Romanello M, Di Napoli C, Drummond P, et al. The 2022 report of the Lancet Countdown on health and climate change: Health at the mercy of fossil fuels. Lancet 2022;400(10363):1619-1654.
2. Howard C, MacNeill AJ, Hughes F, et al. Learning to treat the climate emergency together: Social tipping interventions by the health community. Lancet Planet Health 2023;7:e251-e264.
3. Lenzen M, Malik A, Li M, et al. The environmental footprint of health care: A global assessment. Lancet Planet Health 2020;4:e271-e279.
4. Tennison I, Roschnik S, Ashby B, et al. Health care’s response to climate change: A carbon footprint assessment of the NHS in England. Lancet Planet Health 2021;5:e84-e92.
5. Cristiano W, Marchi C, di Domenico K et al. The elephant in the room in greenhouse gases emissions: Rethinking healthcare systems to face climate change. A rapid scoping review. Environ Sci Eur 2024; 36, 24.
6. Aftergut K. The truly paperless dermatology office. Arch Dermatol 2008;144:1620.
7. Waters E. End of the roll for examination table paper? Can Fam Physician 2020;66:748-749.
8. Bifero AE, Prakash J, Bergin J. The role of chiropractic adjusting tables as reservoirs for microbial diseases. Am J Infect Control 2006;34:155-157.
9. Odeniyi F, Santos J, Hanley S, et al. Scratching the surface: Detecting the presence of viral pathogens in pediatric primary care clinics. Open Forum Infect Dis 2017;4(suppl 1):S161.
10. Shams AM, Rose LJ, Edwards JR, et al. Assessment of the overall and multidrug-resistant organism bioburden on environmental surfaces in healthcare facilities. Infect Control Hosp Epidemiol 2016;37:1426-1432.
11. Provincial Infection Control Network of British Columbia. British Columbia best practices for environmental cleaning for prevention and control of infections in all healthcare settings and programs: Appendix A. 2016. https://picnet.ca/wp-content/uploads/British-Columbia-Best-Practices-for-Environmental-Cleaning-for-Prevention-and-Control-of-Infections-in-All-Healthcare-Settings-and-Programs.pdf.
12. Infection Prevention and Control Canada. Cleaning and disinfection of non-critical multi-use equipment and devices in community settings. IPAC Canada practice recommendations. Updated January 2018. Accessed 12 July 2023. https://ipac-canada.org/photos/custom/Members/pdf/18Jan_Cleaning_NonCrit_Equip_Comm_Practice_Recomm_final.pdf.
13. Public Health Ontario. Infection prevention and control key principles for clinical office practice during the COVID-19 pandemic. 2nd ed. 2022. Accessed 12 July 2023. www.publichealthontario.ca/-/media/documents/ncov/ipac/2020/09/checklist-assessment-primary-care-spec-walk-in-clinics.pdf.
14. Davis M, Ayeni T, Gayowsky T. Examination table paper [infographic]. 2021. Accessed 12 July 2023. https://hamiltonfht-my.sharepoint.com/:b:/g/personal/tatiana_gayowsky_hamiltonfht_ca/EclbOZjf0C5AgB2C-9xVGbwBBr_npd43jT1fkfI8l9rV-Q.
15. Hop J, Bourgault A, Newberry L. De-implementation: Examination table paper for patients who do not need to disrobe. Accessed 12 July 2023. https://www.acha.org/App_Themes/AM20/documents/Virtual_Posters/hop.pdf.
16. Evans MW Jr, Ramcharan M, Floyd R, et al. A proposed protocol for hand and table sanitizing in chiropractic clinics and education institutions. J Chiropr Med 2009;8:38-47.
17. BC Ministry of Environment and Climate Change Strategy. 2020 B.C. best practices methodology for quantifying greenhouse gas emissions. Victoria: Queen’s Printers, 2021. Accessed 1 December 2023. www2.gov.bc.ca/assets/gov/environment/climate-change/cng/methodology/2020-pso-methodology.pdf.
18. United States Environmental Protection Agency. Greenhouse gas equivalencies calculator. Accessed 1 December 2023. www.epa.gov/energy/greenhouse-gas-equivalencies-calculator.
19. Armellino D, Walsh TJ, Petraitis V, Kowalski W. Assessment of focused multivector ultraviolet disinfection with shadowless delivery using 5-point multisided sampling of patient care equipment without manual–chemical disinfection. Am J Infect Control 2019;47:409-414.
20. Sherman JD, MacNeill AJ, Biddinger PD, et al. Sustainable and resilient health care in the face of a changing climate. Annu Rev Public Health 2023;44:255-277.
Dr Mariano is a medical oncologist practising at BC Cancer – Vancouver. Ms Wells is a research assistant in the Department of Surgery, Faculty of Medicine, University of British Columbia. Dr Brown is a radiologist and co-chair of the BC Cancer Planetary Health Unit. Ms Clement is a resource librarian at BC Cancer – Kelowna and the BC Cancer Planetary Health Unit. Ms Wooffindin is a registered nurse and infection prevention and control practitioner at BC Cancer – Vancouver. Mr Hare is director of operations at BC Cancer and co-chair of the BC Cancer Planetary Health Unit. Dr Lefresne is a radiation oncologist who treats gastrointestinal and thoracic cancers. Ms Kaur is a clinical nurse specialist with the Nursing and Allied Health Research and Knowledge Translation department at BC Cancer. Mr Darud is the director of clinical operations at BC Cancer – Kelowna. Mr Chui is laboratory manager at BC Cancer Research and oversees department operation. Ms Sun is the director of continuous improvement and performance at BC Cancer.

Hello,
Wonderful project!
I work in the Stroke Prevention Clinic Outpatients (Diamond Health Care Centre - VGH) as an RN for twelve neurologists.
We have six exam rooms using table paper between patients.
Our patient population rarely undress for a neuro examination.
If I may I would like to "borrow" your study and present it to my clinic for review.
I believe it would work and could invest the physicians to change their practice from paper to an appropriate sanitizing solution for the exam tables.
Thank you very much for conducting this study and spotlighting the terrific outcomes you present.
Kind regards,
Yolanda