Does the albumin:creatinine ratio lack clinical utility in predicting microalbuminuria?
Issue: BCMJ,
vol. 48 , No. 8 , October 2006 ,
Pages 399-403 Clinical Articles
Background: The albumin:creatinine ratio and the albumin excretion rate are both used to screen for microalbuminuria and to determine if renal function is declining. As well as having the option of two main screening methods in British Columbia, we have two different reference ranges, one used by community labs and one recommended by the Canadian Diabetes Association.
Methods: To investigate the ability of the albumin:creatinine ratio to accurately predict microalbumin levels we studied 109 consenting outpatients from the St. Paul’s Hospital Diabetes Centre. Subjects had at least a 5-year history of diabetes mellitus and negative or trace protein in their most recent urinalysis. They each provided a spot morning urine sample at a community lab and a 24-hour urine sample. The albumin:creatinine ratio results obtained from the spot sample were then compared with the albumin excretion rate results obtained from the 24-hour sample using Canadian Diabetes Association reference ranges.
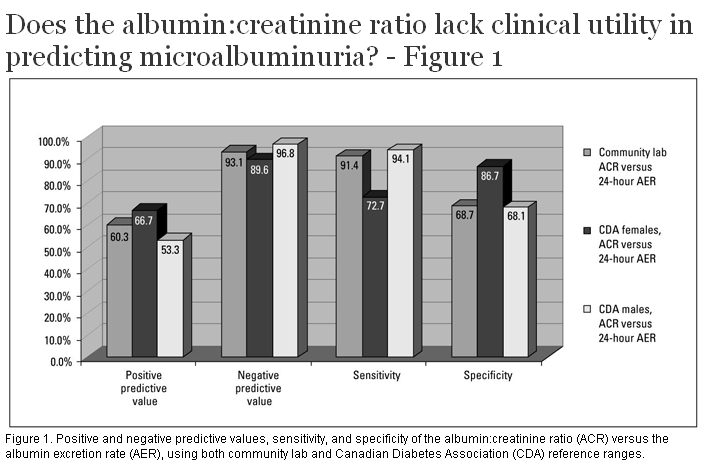
Results: Based on the community lab’s reference ranges, the albumin:creatinine ratio was found to have a positive predictive value of 0.603, a negative predictive value of 0.931, a specificity of 0.687, and a sensitivity of 0.944 when compared with the 24-hour albumin excretion rate.
Conclusions: The reference ranges recommended by the Canadian Diabetes Association provide albumin:creatinine ratio results that lack sensitivity and specificity. More important, the albumin:creatinine ratio does not consistently identify patients with microalbuminuria and the 24-hour albumin excretion rate should be used instead for this purpose.
This study finds that the albumin:creatinine ratio is less accurate than the 24-hour albumin excretion rate when assessing the possibility of reduced renal function in diabetic patients.
Diabetic nephropathy is currently the leading cause of end-stage renal disease in the western world. This makes being able to determine when renal function is on the decline of vital importance and explains why tests to identify clinical microalbuminuria have become standard for screening[1] and treating nephropathy in patients with type 1 and type 2 diabetes mellitus. Between 10% and 45% of patients with microalbuminuria progress to proteinuria,[2,3] while 40% can revert to normoalbuminuria with control of hyperglycemia and hypertension.[4]
The two main methods used to determine if a patient is microalbuminuric are the 24-hour albumin excretion rate (AER) and the albumin:creatinine ratio (ACR). Because of the inconvenience of 24-hour urine collection, the ACR has been adopted to estimate urine albumin excretion rates. The ACR has been shown to be convenient, cost-effective, and efficient in screening patients for microalbuminuria when compared with 24-hour collections;[5] however, there is a lack of consistent comparisons between the ACR and 24-hour AER. Currently, the ACR is used extensively to determine the presence of microalbumin and has even been utilized as a gold standard when ascertaining the efficacy of other diagnostic tests.[6,7]
Numerous studies have documented the correlation of ACR results with 24-hour AER results.[5,8,9] Chaiken and colleagues obtained a correlation of r = 0.96 when comparing untimed morning ACR results with 24-hour AER results.[5] However, most studies involve subjects with clearly elevated albumin levels (>30 mg/24 hours). For instance, a study obtaining a correlation of r = 0.89[10] was based on patients with an average AER of 55.7±18.2 mg/24 hours and an ACR of 4.46±1.28 mg/mmol—values well above the Canadian Diabetes Association (CDA) reference ranges for microalbuminuria.
Recent studies have also examined the intraindividual variation in AER. A study by Gomes and Goncalves examined intraindividual variation in normoalbuminuric patients compared with patients who were intermittently microalbuminuric (they had one out of three results that were AER microalbuminuric: 30–300 mg/24 hours) versus patients who were persistently microalbuminuric. The largest intraindividual variation was found in the intermittently microalbuminuric patients,[11] making the clinical interpretation of patients in this category controversial.
Another potential source of error in interpreting ACR results lies in the reference ranges for normoalbuminuria and microalbuminuria used by community labs and the gender-specific ranges used by the Canadian Diabetes Association. The validation of the CDA ranges using community lab reference ranges is unknown.[12]
This study was conducted to investigate whether the ACR is clinically accurate in patients in the intermittent stages of microalbuminuria, and to evaluate the effect of using different reference ranges when screening is based on ACR results.
All patients were recruited through the Diabetes Centre at St. Paul’s Hospital and signed informed consent forms. A total of 109 patients (17 type 1, 92 type 2) were recruited for the study. The St. Paul’s Hospital Ethics Committee approved the study protocol. Participants were included based on having a minimum 5-year history of diabetes mellitus and a negative or trace amount of protein in their urine as measured by dipstick urinanalysis.
Subjects visited any MDS Metro community laboratory in Vancouver before 10 a.m. and provided a urine sample. At this time they were given a container to collect their 24-hour urine samples. No specific instructions were given for fluid intake, physical exercise, or dietary protein intake. Subjects were asked to delay participating if they were menstruating or had urinary tract infections at the time. They were also asked to store the sample in the refrigerator and to add their last void of the 24-hour collection to the sample and return it to the same community lab. Although samples were obtained at various community labs throughout Vancouver, they were all analyzed in the same central laboratory.
The spot urine sample was analyzed to obtain the ACR value, and the 24-hour sample was analyzed to obtain creatinine and albumin values. Urinary albumin and creatinine were measured using the Cobas Integra system (Roche Diagnostics). Urinary albumin was measured by the immunoturbidimetric method. Urinary creatinine was measured by the kinetic Jaffe reaction. Patient results were excluded from the study if creatinine excretion was not within the lab’s reference range of 7.1 to 17.7 mmol/day.
The ACR was then measured against the 24-hour AER. The 24-hour AER was taken to be the gold standard assessment of microalbumin excretion. Positive and negative predictive values, sensitivity, and specificity were then calculated based on the reference ranges in the Table .
The 109 participants (65 male, 44 female) in the study had an average hemoglobin A1c at entry of 7.4±1.2%. According to each patient’s most recent dipstick urinalysis prior to participating in the study, 103 patients had negative protein and 6 patients had trace amounts of protein (<0.3 g/L). The mean patient age was 62.2±12.2 years, and average duration of diabetes mellitus was 15.3±9.6 years. Seven of the 109 patients were excluded: three patients failed to have an AER analysis completed, and four patients had a creatinine value outside of the protocol range.
Using the community lab’s reference ranges (1.7 mg/mmol for the ACR and 21.6 mg/24 hours for the AER) we obtained the positive and negative predictive values, sensitivity, and specificity of the ACR in the prediction of 24-hour AER that are displayed in the Figure . The results presented indicate that when given a population of people with diabetes mellitus who show negative or trace protein in urinalysis and no urinary tract infection, between 25% and 45% of those who have had an ACR test performed will be miscategorized as having microalbumin excretion when, in fact, microalbumin is not present. In addition, between 5% and 11% of the population will not have microalbumin excretion recognized when it is present.
The ACR has poor specificity (68.7%) and a low positive predictive value (60.3%), irrespective of gender, when compared with 24-hour AER samples using a community lab’s reference range. When gender-specific Canadian Diabetes Association reference ranges are considered, specificity remains poor for men (68.1%) while appearing somewhat better for women (86.7%). Several previous studies have found specificities in the low-80% range for the ACR,[13-15] but ours is the first to demonstrate such a poor specificity for the ACR versus the 24-hour AER. In the case of positive predictive value, it remains low when men (59.3%) and women (66.7%) are considered separately. This finding confirms previous research by Lepore and colleagues, who found that the low positive predictive value (68.2%) of the ACR impeded its ability to determine AER.[16] Similarly, Hutchison and colleagues reported a positive predictive value of 77.8%.[17] In addition, using a study design similar to ours, Houlihan and colleagues reported positive predictive values of 68.9% (men) and 86.3% (women).[13] These findings demonstrate that the performance of the ACR as an estimate of microalbumin excretion was suboptimal when compared with the 24-hour AER. A major implication of these results is that a decision to prescribe lifelong medication in an effort to prevent nephropathy may be wrong one-third of the time.
The ACR did have a high negative predictive value, indicating that the ACR is useful in determining when patients are normoalbuminuric, but it still cannot be relied on when making a therapeutic decision such as diagnosing early stage diabetic nephropathy.
A review of the literature regarding microalbumin excretion revealed a high degree of variability between studies. Some studies compared the ACR to an overnight AER,[14,16,18-20] while others used 24-hour AER.[13,15] In addition, some studies used first void samples for calculating ACR[14,16,18,21] while others used random collection urine samples in their calculation of ACR.[13,20] Due to this variability in study design, a range of sensitivities from 80% to 100% were obtained. The high degree of variability among study results makes any conclusions about the efficacy of the ACR difficult to generalize.
An increased sensitivity (94.1%) was observed in males using Canadian Diabetes Association reference ranges. Female ACR analysis resulted in a high specificity (86.7%) and low sensitivity (72.7%), indicating that the ACR is more accurate in identifying microalbuminuria in a male population. This gender difference is in contrast to results from a previous study, which found that the ACR has a high ability to predict microalbuminuria in both men and women.
Additional influencing factors
The inability of the ACR to predict microalbuminuria may be due in part to variations in urine volume, which affects the concentration of creatinine and/or albumin within a sample. As a result, inconsistent urine collection in random samples can result in increased variability in ACR results.[18] Measuring urinary creatinine is a technique to correct for variations in urine collection; however, the measurement of creatinine can itself be a source of variability.[22] The creatinine excretion rate depends on a stable glomerular filtration rate.[10] In microalbuminuric patients, the glomerular filtration rate can be altered and the creatinine variability can be increased. The coefficient of variation for urinary creatinine can be increased by as much as 25%.[19] Furthermore, creatinine excretion is influenced by age. Recent research has shown that as age increases, creatinine excretion decreases. Thus, an age-adjusted ACR could result in a higher specificity.[21] Also, the variability of creatinine and albumin excretion is compounded by small sample size, which can result in increased variability in estimates of albumin excretion.
Along with variability in urine volume, a number of physiological and pathological conditions can affect microalbumin excretion rates. Elevated urinary excretion of albumin can vary as a result of exercise, pregnancy, febrile illness, inflammation, urinary tract infections, slight urinary tract bleeding, or benign postural proteinuria.[23] Compounding this, polyuria, hyperglycemia, and hypertension can alter microalbumin excretion.[19,24] The diurnal variation in AER results in a 30% to 50% lower AER during the night,[23] which indicates that a spot sample may be affected by the time it is taken and thus may not be consistent with 24-hour AER results. Fluctuating microalbumin excretion potentially contributes to decreased agreement between spot sample ACR and 24-hour AER results. Microalbumin variation is determined by two parameters: albumin passage over the glomerular membrane and tubular reabsorption. It has been well documented that the coefficient of variation for urinary albumin excretion is between 30% and 50%.[19]
Using results from a community lab we have demonstrated the inadequacy of the albumin:creatinine ratio as an alternative to the 24-hour albumin excretion rate in diagnosing microalbuminuria. Furthermore, we have illustrated that the current reference ranges recommended by the Canadian Diabetes Association fail to provide ACR results with adequate sensitivity and specificity. We recognize that Canadian Diabetes Association clinical practice guidelines state that two out of three tests over 3 months must be positive to confirm a positive result;[11] however, a review of the literature found no support for this consensus-based recommendation. Additionally, we know that clinical decisions are often based on a single positive ACR result.
Thus, while the ACR appears to have utility in predicting normal microalbumin excretion as evidenced by a single negative ACR having significant negative predictive value (>90%), the utility of the ACR in predicting true microalbumin excretion is low. To predict true microalbumin excretion, a 24-hour AER is required. Using the AER rather than the ACR can help physicians accurately categorize patients and can prevent misdiagnosis, unnecessary treatment, and undiagnosed proteinuria.
Acknowledgments
We would like to thank the Endocrine Research Society of Vancouver for funding this project.
Competing interests
This study was funded entirely by the Endocrine Research Society. In the past, Dr Tildesley has received funds for unrelated projects and for speaking from numerous companies, including GlaxoSmithKline, Eli Lilly, Pfizer, Servier, and Novo.
Table. Normal reference ranges used by a community lab and recommended by the Canadian Diabetes Association (CDA) to screen for microalbuminuria
| Albumin:creatinine ratio (mg/mmol) | Albumin excretion rate (mg/24 hours) | Protein excretion rate (g/24 hours) | |
| Community lab reference ranges | <1.70 | <21.60 | <0.15 |
| CDA reference ranges, females | <2.80 | <30.00 | <0.15 |
| CDA reference ranges, males | <2.00 | <30.00 | <0.15 |
References
1. Mangili R. Microalbuminuria in diabetes. Clin Chem Lab Med 1998;36:941-946. PubMed Abstract
2. Caramori ML, Fioretto P, Mauer M. The need for early predictors of diabetic nephropathy risk: Is albumin excretion rate sufficient? Diabetes 2000;49:1399-1408. PubMed Abstract Full Text
3. Bruno G, Merletti F, Biggeri A, et al. Progression to overt nephropathy in type 2 diabetes. The Casale Monferrato Study. Diabetes Care 2003;26:2150-2155. PubMed Abstract Full Text
4. Perkins BA, Ficociello LH, Silva KH, et al. Regression of microalbuminuria in type 1 diabetes. N Engl J Med 2003;348:2285-2293. PubMed Abstract Full Text
5. Chaiken RL, Khawaja R, Bard M, et al. Utility of untimed urinary albumin measurements in assessing albuminuria in black NIDDM subjects. Diabetes Care 1997;20:709-713. PubMed Abstract
6. Lum G. How effective are screening tests for microalbuminuria in random urine specimens? Ann Clin Lab Sci 2000;30:406-411. PubMed Abstract
7. Tabaei BP, Al-Kassab AS, Ilag LL, et al. Does microalbuminuria predict diabetic nephropathy? Diabetes Care 2001;24:1560-1566. PubMed Abstract Full Text
8. Nathan DM, Rosenbaum C, Protasowicki VD. Single void urine samples can be used to estimate quantitative microalbuminuria. Diabetes Care 1987;10:414-418. PubMed Abstract
9. Marshall SM. Screening for microalbuminuria: Which measurement? Diabet Med 1991;8:706-711. PubMed Abstract
10. Assadi F. Quantification of microalbuminuria using random urine samples. Pediatr Nephrol 2002;17:107-110. PubMed Abstract
11. Gomes MB, Goncalves MF. Is there a physiological variability for albumin excretion rate? Study in patients with diabetes type 1 and non-diabetic individuals. Clin Chem Acta 2001;304:117-123. PubMed Abstract
12. Meltzer S, Leiter L, Daneman D, et al. 1998 clinical practice guidelines for the management of diabetes in Canada. Canadian Diabetes Association. CMAJ 1998:159(suppl 8):S1-S29. PubMed Abstract Full Text
13. Houlihan CA, Tsalamandris C, Akdeniz A, et al. Albumin to creatinine ratio. A screening test with limitations. Am J Kidney Dis 2002;39:1183-1189. PubMed Abstract Full Text
14. Gatling W, Knight C, Hill RD. Screening for early diabetic nephropathy: Which sample to detect microalbuminuria? Diabet Med 1985;2:451-455. PubMed Abstract
15. Wiegmann TB, Chonko AM, Barnard MJ, et al. Comparison of albumin excretion rate obtained with different times of collection. Diabetes Care 1990;13:864-871. PubMed Abstract
16. Lepore G, Maglio ML, Nosari I, et al. Cost-effectiveness of two screening programs for microalbuminuria in type 2 diabetes. Diabetes Care 2002;25:2103. PubMed Citation Full Text
17. Hutchison AS, O’Reilly DJ, MacCuish AC. Ablumin excretion rate, albumin concentration, and albumin/creatinine ratio compared for determining diabetics for slight albuminuria. Clin Chem 1988;34:2019-2021. PubMed Abstract
18. Zelmanovitz T, Gross JL, Oliveira JR, et al. The receiver operating characteristics curve in the evaluation of a random urine specimen as a screening test for diabetic nephropathy. Diabetes Care 1997;20:516-519. PubMed Abstract
19. Mogensen CE, Vestbo E, Poulsen PL, et al. Microalbuminuria and potential confounders. A review and some observations on variability of urinary albumin excretion. Diabetes Care 1995;18:572-581. PubMed Citation
20. Gatling W, Knight C, Mullee MA, et al. Comparison of albumin excretion rate obtained with different times of collection. Diabetes Care 1988;5:343-347.
21. Watts GF, Shaw KM, Polak A. The use of random urine samples to screen for mircoalbuminuria. Diabetes Care 1987;10:414-418.
22. Mattix HJ, Hsu CY, Shaykevich S, et al. Use of the albumin/creatinine ratio to detect microalbuminuria: Implications of sex and race. J Am Soc Nephrol 2002;13:1034-1039. PubMed Abstract Full Text
23. Emancipator K. Laboratory diagnosis and monitoring of diabetes mellitus. Am J Clin Pathol 1999;112:665-674. PubMed Abstract
24. Viberti BG, Mogensen CE, Keen H, et al. Urinary excretion of albumin in normal man: The effect of water loading. Scand J Clin Lab Invest 1982;42:147-157. PubMed Abstract
Kevin W. Johns, BSc, Claire E. Robinson, BSc, Ian M. Wilson, BMLSc, Emma O. Billington, BSc, Greg P. Bondy, MD, Hugh D. Tildesley, MD
Mr Johns, Ms Robinson, Mr Wilson, and Ms Billington are research assistants, Diabetes Research, Division of Endocrinology, at St. Paul’s Hospital, Vancouver, British Columbia. Dr Bondy is clinical associate professor of medicine and pathology at UBC and associate director of the Lipid Clinic at at the Healthy Heart Program at St. Paul's Hospital. Dr Tildesley is an endocrinologist at St. Paul’s Hospital and a clinical associate professor in the Department of Medicine at the University of British Columbia.

{kind=link}