Delirium after cardiac surgery: A retrospective case-control study of incidence and risk factors in a Canadian sample
Issue: BCMJ,
vol. 51 , No. 5 , June 2009 ,
Pages 206-210 Clinical Articles
Background:Postoperative delirium is a major complication of cardiac surgery. A pilot study was proposed to determine the incidence of delirium and identify risk factors for delirium in patients undergoing elective heart surgery in a Canadian hospital.
Methods:Charts of 38 patients admitted for heart surgery were reviewed retrospectively. Variables related to delirium were characterized as being present before, during, or after cardiac surgery. Logistic regression was used to calculate odds ratios for risk factors.
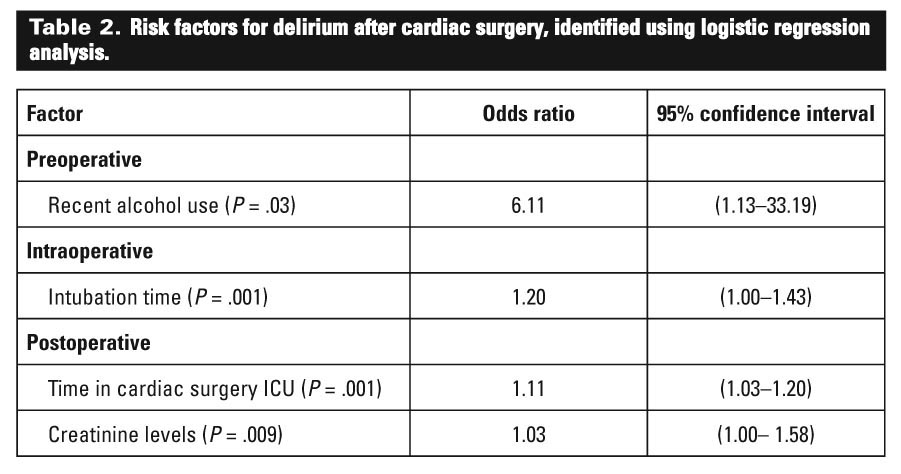
Results:After cardiac surgery 11 of 38 patients developed delirium. The risk factor associated most strongly with delirium was recent alcohol use (OR 6.11), followed by intubation time (OR 1.20), time spent in intensive care (OR 1.11), and postoperative creatinine levels (OR 1.03).
Conclusions:The incidence of delirium following cardiac surgery is considerable, with almost one-third of patients becoming delirious. Special attention should be paid to alcohol use in the period preceding surgery and future studies should look specifically at alcohol use and dependence as risk factors for delirium after cardiac surgery.
Alcohol use in the week before surgery was identified as the risk factor most strongly associated with postoperative delirium in a recent study at St. Paul’s Hospital.
Background
Postoperative delirium is a common complication of cardiac surgery.[1] Episodes of delirium are associated with increased morbidity, mortality, and a longer hospital stay[2,3] and can be distressing for patients, their families, and nursing staff.[4] Recognizing delirium and those at risk can reduce the impact of delirium through targeted interventions and risk reduction.[5,6] Understanding the frequency of delirium and the complications associated with it can help guide future research and resource allocation.
Historically, a number of psychiatric symptoms have been identified following heart surgery: confusion, agitation, and hallucinations have been labeled postcardiotomy delirium,[1] postoperative psychosis,[7] and acute brain syndrome.[8] Earlier studies of postoperative patients did not define delirium in a consistent way because a standard definition has only been available since the publication of the DSM-III.[9]
Most of the surgeries described in the earliest reports involved repairing valves and congenital anomalies.[8] Coronary artery bypass graft (CABG) is now the most common type of cardiac surgery[10,11] and may have lower rates of delirium than valve surgery.[8] Nevertheless, in Canada, bypass grafts and other types of cardiac surgery are increasingly being performed on patients who are older and have a greater number of comorbid medical conditions,[12] which may make them more at risk for delirium. While the mortality from cardiac operations in British Columbia is decreasing,[12] it is unclear whether the incidence of delirium is as well. Despite the development of a consistent definition of delirium and standardized measurements for it, there are significant discrepancies between studies on the incidence of delirium,[11] making it difficult to predict what rates of delirium will occur in a given population.
The study described here was designed to determine the incidence of postoperative delirium and to identify risk factors by taking advantage of the extensive data collected on cardiac surgery patients in British Columbia. These patients receive preoperative screening by anesthesiologists and nurses. Data about each case—including variables that have been identified as risk factors for delirium in other studies—are gathered from the preoperative, intraoperative, and postoperative period and entered into a provincial health database.
Methods
Patients
Study subjects were chosen by reviewing a consecutive series of charts for patients undergoing elective heart surgery during a 2-week period in 2007 at St. Paul’s Hospital, a tertiary care facility in Vancouver, BC. Thirty-eight patients were selected for the study. All procedures were approved by the University of British Columbia Clinical Research Ethics Board.
Data input and gathering
Before surgery, a preoperative assessment of each patient was performed by an anesthesiologist and cardiac nurse. The assessment involved the use of standardized screening questionnaires that included a number of questions about risk factors for delirium, as well as standardized questions about regular alcohol consumption and consumption during the week before surgery. Intraoperative data were gathered along with postoperative data recorded by nursing staff in the cardiac intensive care unit and the postoperative medical unit. Following the presentation of delirium, additional variables that were of clinical interest, such as frequency of psychiatrist consultation, were also recorded even though these could not have contributed to the onset of delirium. The data gathered are displayed in Table 1.
{kind=link}
Delirium assessment
The diagnosis of delirium was based on DSM-IV-TR[13] criteria and was made retrospectively using progress notes. The nurses had been trained in using the confusion assessment method (CAM)[14] to screen for and diagnose delirium. A patient was deemed to have delirium if the DSM-IV-TR criteria were met according to the progress notes, if the patient’s CAM rating was positive, or if the diagnosis was made by a physician involved in the patient’s care.
Statistics
Group differences comparing variables between patients with or without delirium were analyzed with independent-means t tests for continuous variables and the chi-square test for dichotomous variables. Because of the relatively small sample size, risk factors for delirium at the preoperative, intraoperative, or postoperative stages were selected from Table 1 only if there was a significant between-group difference (P <.05) as determined by forward stepwise logistic regression analysis. SPSS software was used for all analyses.
Results
The majority of patients undergoing surgery were male (78.9%) and the mean age was 67 years. The surgical interventions included CABG alone in 22 cases, valve surgery in 9 cases, and combined CABG and valve surgery in 7 cases. Three of 38 cases had “off pump” procedures. Patients became delirious in 11 of 38 cases (28.9%). Separate preoperative, intraoperative, and postoperative variables were included in the analysis to determine risk factors for delirium. After logistic regression, four factors were identified as significant predictors of delirium. Alcohol use in the week before surgery, intubation time, time spent in the cardiac surgery intensive care unit, and postoperative creatinine levels were all independently associated with delirium (Table 2).
{kind=link}
The risk factor associated most strongly with delirium was alcohol use in the week preceding admission (OR 6.11). Alcohol use was reported on a standardized questionnaire given to all patients prior to surgery; regular alcohol consumption, irrespective of use in the week preceding admission, was not associated with delirium. Psychiatrists were consulted for 9 of the 11 patients with delirium (82%) and only 2 of the 27 patients without delirium (7%) (x2 = 20.3; P <.001). The postoperative stay was significantly longer for patients with delirium—a mean of 9.7 days versus 6.2 days for patients without delirium (t = 2.64; P = .01). Restraints were used for only 3 of the 11 delirious patients and there were no reported behavioral disturbances or reports of violence toward staff in any of the charts that were reviewed.
Conclusions
Slightly under one-third of the patients in this retrospective case-control study developed delirium after cardiac surgery. Because delirium was diagnosed retrospectively, we may have underestimated its incidence since delirium often goes unrecognized and unrecorded, particularly in cases involving the hypoactive subtype.[15] Nevertheless, the incidence in our study falls well within the range of incidence reported in prospective studies,[3,6,16,17] and is consistent with an incidence of 32% recorded in the only previous prospective study that assessed risk factors for delirium and CABG in a Canadian sample.[18] The rate of psychiatric consultation was high (82%) in the delirious patients, which we believe reflects the awareness of delirium and its impact in our centre.
The factors most strongly associated with delirium were recent alcohol use, intubation time, time spent in the ICU, and postoperative creatinine levels. We suspect that recent alcohol use may precipitate a withdrawal-related delirium, and we believe that ours is the first study to identify recent alcohol use as a strong risk factor specifically for delirium associated with cardiac surgery. A previous major study reported that a history of excessive alcohol use (defined as including “hospitalization resulting from alcohol consumption or withdrawal”) was a risk factor for postcardiac surgery type II cerebral outcome.[19] That study did not assess recent alcohol use, however, and was not specific to delirium, as it included any type of cognitive deterioration, including memory impairment and seizures. All patients at our centre who are considered to be at risk of withdrawal are put on a protocol that includes using the revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scale.[20] Given the relative risk for delirium in recent drinkers, future studies should assess the amount, duration, and regularity of alcohol use, as well as any history of withdrawal symptoms.
We did not find a significant association with a number of factors that we anticipated would be associated with delirium. We reviewed postoperative doses of opioids and benzodiazepines, suspecting that these medications might be associated with delirium,[21] but we did not find evidence for this. We were also interested in “code white” calls and violent incidents, as these are particularly concerning events for staff and patients: no calls or incidents were reported with any of the patients.
Caution should be made when attributing cause to associated factors. Because delirium results from a complex interaction of factors, it is difficult to determine which of the factors are causal and which are a result of confounding common underlying pathology. For example, longer intubation time will predispose an individual to a respiratory infection[22] that can then contribute to delirium.[23] It is also possible that the more severely ill patients and those with more complications in surgery would be likely to have both longer intubation times and higher rates of delirium with no connection between the two.
As this pilot study involved only 38 patients, the statistical power to detect differences between those who developed delirium and those who did not was modest. This may account for the study’s inability to identify previously reported risk factors, such as age[24] or prior stroke.[18] However, a study with a small sample size also offers some benefits, including the strength of the association in those variables that are identified, highlighting risk factors for delirium that are clinically relevant. Future prospective studies that consider larger numbers of subjects, that use standardized measures, and that take into account the severity and consequences of delirium are warranted. Additionally it may be useful to conduct studies that look specifically at alcohol consumption and dependence as risk factors.
Acknowledgments
We are indebted to the Consultation-Liaison service at St. Paul’s Hospital, including Dr Alan Burgman, Dr Stephen Fitzpatrick, and Dr Carole Richford. Their consultation and input into the study were invaluable.
Competing interests
None declared.
References
1. Blachy PH, Starr A. Post-cardiotomy delirum. Am J Psychiatry 1964;121:371-375. Abstract
2. Bucerius J, Gummert JF, Borger MA, et al. Predictors of delirium after cardiac surgery delirium: Effect of beating-heart (off-pump) surgery. J Thorac Cardiovasc Surg 2004;127:57-64. PubMed Abstract
3. McKhann GM, Grega MA, Borowicz LM Jr, et al. Encephalopathy and stroke after coronary artery bypass grafting: Incidence, consequences, and prediction. Arch Neurol 2002;59:1422-1428. Full Text
4. Breitbart W, Gibson C, Tremblay A. The delirium experience: Delirium recall and delirium-related distress in hospitalized patients with cancer, their spouses/caregivers, and their nurses. Psychosomatics 2002;43:183-194. Full Text
5. Inouye SK. Prevention of delirium in hospitalized older patients: Risk factors and targeted intervention strategies. Ann Med 2000;32:257-263. PubMed Abstract
6. Marcantonio ER, Flacker JM, Wright RJ et al. Reducing delirium after hip fracture: A randomized trial. J Am Geriatr Soc 2001;49:516-522. Abstract
7. Sveinsson IS. Postoperative psychosis after heart surgery. J Thorac Cardiovasc Surg 1975;70:717-726. PubMed Abstract
8. Rabiner CJ, Willner AE, Fishman J. Psychiatric complications following coronary bypass surgery. J Nerv Ment Dis 1975;160:342-348. PubMed Abstract
9. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: APA; 1980.
10. Northrup WF 3rd, Emery RW, Nicoloff DM, et al. Opposite trends in coronary artery and valve surgery in a large multisurgeon practice, 1979-1999. Ann Thorac Surg 2004;77:488-495. Full Text
11. Sockalingam S, Parekh N, Bogoch II, et al. Delirium in the postoperative cardiac patient: A review. J Card Surg 2005;20:560-567. Abstract
12. Ghali WA, Quan H, Shrive FM, et al. Outcomes after coronary artery bypass graft surgery in Canada: 1992/93 to 2000/01. Can J Cardiol 2003;19:774-781. PubMed Abstract
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th rev ed. Washington, DC: APA; 2000.
14. Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113:941-948. PubMed Abstract
15. Eriksson M, Samuelsson E, Gustafson Y, et al. Delirium after coronary bypass surgery evaluated by the organic brain syndrome protocol. Scand Cardiovasc J 2002;36:250-255. PubMed Abstract
16. Kazmierski J, Kowman M, Banach M, et al. Preoperative predictors of delirium after cardiac surgery: A preliminary study. Gen Hosp Psychiatry 2006;28:536-538. PubMed Abstract
17. Calabrese JR, Skwerer RG, Gulledge AD, et al. Incidence of postoperative delirium following myocardial revascularization. A prospective study. Cleve Clin J Med 1987;54:29-32. PubMed Abstract
18. Rolfson DB, McElhaney JE, Rockwood K, et al. Incidence and risk factors for delirium and other adverse outcomes in older adults after coronary artery bypass graft surgery. Can J Cardiol 1999;15:771-776. PubMed Abstract
19. Roach GW, Kanchuger M, Mangano CM, et al. Adverse cerebral outcomes after coronary bypass surgery. Multicenter Study of Perioperative Ischemia Research Group and the Ischemia Research and Education Foundation Investigators. N Engl J Med 1996;335:1857-1863. Full Text
20. Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: The revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict 1989;84:1353-1357. PubMed Abstract
21. Jackson N, Doherty J, Coulter S. Neuropsychiatric complications of commonly used palliative care drugs. Postgrad Med J 2008;84:121-126; quiz 125. Full Text
22. Miyamoto T, Kimura T, Hadama T. The benefits and new predictors of early extubation following coronary artery bypass grafting. Ann Thorac Cardiovasc Surg 2000;6:39-45. PubMed Abstract
23. Hanson MR, Galvez-Jimenez N. Management of dementia and acute confusional states in the perioperative period. Neurol Clin 2004;22:vii-viii, 413-422. PubMed Abstract
24. Loponen P, Luther M, Wistbacka JO, et al. Postoperative delirium and health related quality of life after coronary artery bypass grafting. Scand Cardiovasc J 2008;42:337-344. PubMed Abstract
Dr Burns is a psychiatrist in the Department of Psychiatry at the University of British Columbia. Dr Jenkins is a first-year resident in the postgraduate psychiatry program at UBC. Mr Yeh is a third-year medical student at UBC. Dr Procyshyn is a clinical associate professor in the Department of Psychiatry at UBC and a research scientist at the BC Mental Health and Addictions Research Institute. Dr Schwarz is anesthesia research director at St. Paul’s Hospital and the recipient of a Canadian Anesthesiologist’s Society/Abbott Laboratories Ltd. career scientist award in anesthesia. Dr Honer is a professor in the Department of Psychiatry at UBC and scientific director of the BC Mental Health and Addictions Research Institute. Dr Barr is an assistant professor in the Department of Anesthesiology, Pharmacology & Therapeutics at UBC, as well as a Michael Smith Foundation for Health Research scholar and a Canadian Institutes of Health Research new investigator.