A case of cutaneous myiasis in British Columbia
Issue: BCMJ,
vol. 59, No. 9, November 2017,
Pages 450-453 Clinical Articles
ABSTRACT: Cutaneous myiasis, the infestation of a parasite in the skin, is rarely considered in patients who have traveled solely within North America. While there have been case reports in other parts of Canada, this report outlines the first documented case treated in British Columbia. An 18-month-old toddler, initially misdiagnosed with preseptal cellulitis, was found to have a supraorbital lesion containing a larva of the genus Hypoderma. Relevant clinical history included recent contact with livestock, insect bites surrounding the affected area, and reports of movement within the lesion. On examination, inspecting for a central punctum and observing for larval protrusion was essential for diagnosis. Applying an occlusive dressing can aid in visualization and extraction. Practitioners should familiarize themselves with the signs and symptoms of myiasis and consider this diagnosis for patients in Canada.
A pediatric patient who was initially treated for a swollen eyelid following a family camping trip to Ontario and Quebec was eventually diagnosed with cutaneous myiasis. This first documented Canadian-acquired case in BC is a reminder that practitioners should be familiar with the signs and symptoms of myiasis.
Myiasis describes the parasitic infestation of a host, such as a human or other vertebrate, with larvae from the order Diptera (flies).[1-3] Cutaneous myiasis, the infestation of a parasite in the skin, commonly occurs in travelers to tropical and subtropical latitudes.[2,3] This diagnosis is not often considered in patients who have traveled solely within North America. However, there have been many case reports of cutaneous myiasis in temperate regions of North America, including Canada.[2,4-6] This report outlines the first documented case of Canadian-acquired cutaneous myiasis treated in British Columbia. Due to their rarity, cases of myiasis are often misdiagnosed, leading to ongoing patient discomfort and delay in an otherwise simple treatment. Practitioners should familiarize themselves with the signs and symptoms of myiasis and consider this diagnosis for patients in Canada.
Case description
An 18-month-old fully-immunized, previously healthy caucasian female presented to the emergency department in Victoria, BC, with a swollen left eyelid. Three days prior, she and her family had returned from an 8-day camping trip to Poltimore, Quebec, and Stittsville, Ontario. Her parents described an otherwise well toddler with no fevers, no discomfort, and no intraocular signs or symptoms. On examination, there was a well-demarcated erythematous swelling surrounding the left eye. Additionally, there were several small papules surrounding this area resembling insect bites (Figure 1). There was no chemosis or proptosis, no conjunctival erythema, and her extraocular movements were normal and nonpainful. The lesion was swabbed for culture and sensitivity, which showed only skin flora, and the patient was empirically treated for preseptal cellulitis with a 10-day course of oral amoxicillin and trimethoprim-sulfamethoxazole.
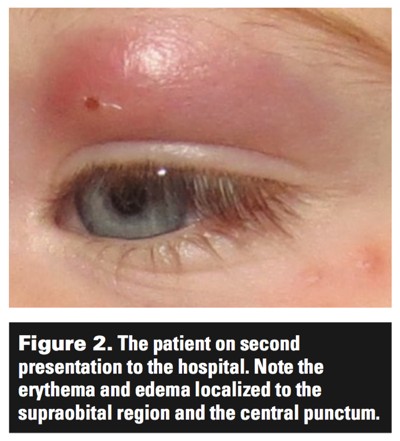
Eleven days later the patient returned to the emergency department with nonresolving symptoms. On examination, the erythema and papules below the left eye had resolved. However, the supraorbital lesion had grown significantly to form a fluctuant draining mass, or furuncle, 2 cm above the left eyelid. The lesion had a central punctum, which the parents reported had developed over the last few days (Figure 2). The parents described purulent drainage from the punctum as well as an intermittently protruding foreign body. The patient continued to have normal extraocular movements and was systemically well.
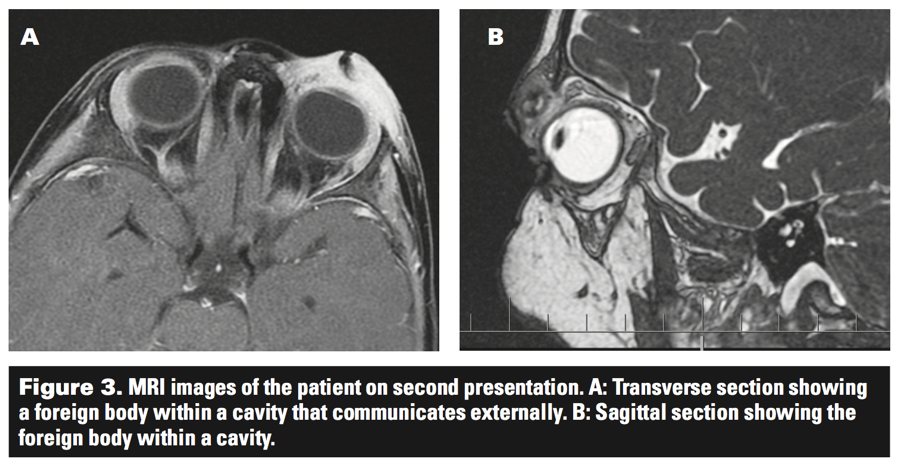
The patient was admitted to hospital for further investigations, observation, and empiric treatment with antibiotics. Movement within the punctum as described by parents was observed, and consideration was given to a possible calvarial defect, sinus fistula, or mobile foreign body. An MRI of the head and orbit revealed a noncommunicating cavity containing a mass presumed to be a foreign body, as well as significant preseptal cellulitis (Figure 3). At this point, suspicion was high for the presence of a larva.
Petroleum jelly and occlusive dressing were applied a few minutes prior to the procedure to suffocate the organism and induce protrusion to facilitate removal. The patient was taken to the procedure room and sedated. Once the dressing was removed the organism protruded. It was then grasped with forceps and, using gentle traction, removed intact without difficulty. Using manual pressure, serosanguinous fluid was expressed from the tract. The patient tolerated the procedure well, and she was discharged the following day with oral antibiotics for residual cellulitis.
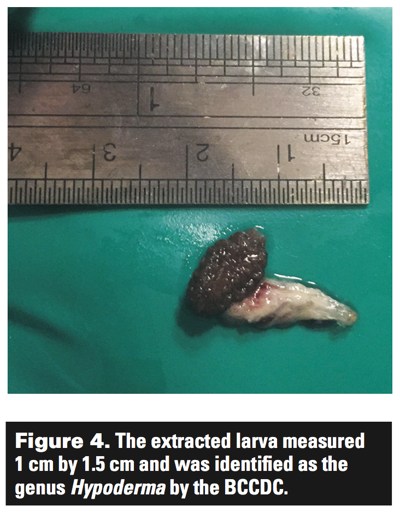
The specimen measured 1 cm by 1.5 cm and was sent to British Columbia Centre for Disease Control (BCCDC) for identification, where it was identified as a larva of the genus Hypoderma (Figure 4).
Myiasis-producing flies
A number of flies (order Diptera) are known to invade human hosts and cause myiasis; the most well known is the human bot fly (Dermatobia hominis).[3] Others include Wohlfahrtia vigil, Cordylobia anthropophaga, and a number of other species.[3,7] While the majority of these organisms are found in tropical climates, therefore locally causing the largest burden of disease, temperate climates are home to a number of species as well. Specifically, cases of myiasis caused by Wohlfahrtia, Hypoderma, Cuterebra, and Sarcophaga species have all been reported in Canada.[2,6] In 2008, Caissie and colleagues reported 95 cases of myiasis that had been acquired in Canada, seven of which were caused by Hypoderma spp.[2]
Hypoderma species (H. lineatum and H. bovis) are more commonly known as cattle grub.[8] They occur naturally in cattle and are found in regions containing livestock between northern Mexico and northern Canada.[8] The life cycle of the parasite in cattle occurs in a seasonal pattern over a period of 9 to 10 months. The adult fly lays its eggs on cattle hair in the summer, and 4 to 7 days later the larvae hatch and crawl down the hair to penetrate the skin. This penetration is irritating and causes local inflammation. The larvae travel through subcutaneous tissue to the esophagus, where they remain and grow until the spring when they migrate to the dorsum of the cattle and re-emerge via the skin.[8] A third species of Hypoderma (H. tarandi) is found in the Arctic and similarly infects caribou.[4]
Types of myiasis
Myiasis is generally classified according to location of infestation: cutaneous (the most common), ocular, nasopharyngeal, urogenital, and intestinal.[1] Cutaneous myiasis can be further differentiated based on its clinical manifestations: furuncular myiasis, wound myiasis, and migratory myiasis.[1,3]
Furuncular myiasis is caused by the species of the order Diptera, such as Dermatobia, Cuterebra, Wohlfartia, and on rare occasions, as in this case, Hypoderma.[1,7] Larvae are brought into contact with the skin by exposure to contaminated foliage, feces, or from the bite of a carrier organism, usually a mosquito.[7] Larvae painlessly infiltrate the dermis through a hair follicle or an insect bite, and localize to a subdermal cavity causing a small red papule.[7] The larva feeds on host tissue to fuel its growth and development, causing a progressively enlarging furuncle, and eventually developing a central punctum through which the larva respires. The local inflammatory reaction commonly presents with symptoms such as pruritus and pain as well as a serosanguinous discharge.[1,2,7] Further, patients may report being able to see movement within the furuncle or experience the sensation of movement. If left untreated, larvae will generally migrate out of the skin, fall to the ground, and pupate.
Wound myiasis describes infection of an open wound or mucous membrane and is generally caused by Wohlfahrtia magnifica, Chrysomya bezziana, or Cochliomyia hominivorax.[1,4,7] None of these species is found natively in Canada; however, travelers to Africa, Asia, and Central and South America may return with wound myiasis.[7]
Migratory myiasis refers to the process by which a parasite moves through its host’s tissue to the site where it ultimately manifests. Hypoderma spp. and Gasterophilus spp. (commonly known as the horse bot fly) have been reported to cause migratory myiasis in humans.[1,8] Most cases of migratory myiasis are mild, and their sole clinical finding is yellow pigment resembling a bruise where the initial penetration of the skin occurred. However, there have been case reports of H. tarandi causing much more severe complications, such as nervous system invasion and vision loss, or ophthalmomyiasis.[4,7]
Discussion
This patient came to have a furuncular myiasis, infected with a larva of the Hypoderma genus, though it is unclear exactly how this occurred. Most often when Hypoderma spp. larvae penetrate human skin, they suffocate and die,[7] and if they do survive they are more commonly reported to cause a migratory myiasis.[1,7] As the skin penetration causes inflammation, we suspect in this case that the larva penetrated the patient’s skin at the time of the “insect bites” appearing. We surmise that the larva remained in the skin and developed into the observed furuncle instead of migrating as reported in similar cases,[9] or as it does in its usual host.
Where the patient came into contact with the larva is also unclear, but considering the time of her travel, it is likely that she acquired the larva while camping in Ontario or Quebec (though we acknowledge that H. lineatum and H. bovis are found widely across the country). There has been another pediatric case of myiasis acquired while camping in Ontario,[6] though we believe this to be the first Canadian-acquired case treated in British Columbia.
The mechanism of acquisition is also up for debate. While traveling, the patient was in contact with horses, rabbits, and domestic dogs. It is likely that she acquired the larva via direct contact with these animals, as cases of Hypoderma spp. myiasis tend to occur in farm children or those who handle cattle.[7] It is also possible that the patient came into contact with a Hypoderma spp. fly that deposited the egg into her hair, where it hatched and subsequently entered her skin. Further, it is possible that she acquired the larva in British Columbia months earlier and did, in fact, have a mild migratory myiasis, where the symptoms of the initial infestation went unnoticed. As there was no pruritis or erythema of the conjunctivae, it is unlikely that the organism entered through the eye.
Recognizing the key signs and symptoms of furuncular myiasis was critical to making an accurate diagnosis in this case. Particularly important were a history of contact with livestock, recent insect bites, and reports of movement within the lesion. Identifying a central punctum and observing larval protrusion provoked by an occlusive ointment were essential examination findings. Applying an occlusive dressing to aid in visualization is the preferred diagnostic test and MRI is, therefore, not usually necessary. Ultimately the diagnosis was confirmed by extracting and identifying the larva.
Extraction is essential to the treatment of furuncular myiasis. A variety of techniques have been used including pressure, traction, and excision.[2] Digital pressure on either side of the punctum or injection of lidocaine deep to the larva can be effective. Forceps extraction can be performed following suffocation with any occlusive substance. Surgical excision is usually reserved for resistant cases or when the larva is dead.[2]
Myiasis can be prevented by avoiding contact with infected hosts such as livestock, taking precautions while outdoors in rural areas (wearing clothing that covers arms and legs), keeping to a routine of adequate personal hygiene, and screening doors and windows to avoid contact with flies.[2] These precautions should be especially extended to young children, who tend to exert less caution when playing outdoors and thus may be more likely to contact hosts or contaminated foliage.
Conclusion
Myiasis, although an uncommon condition in Canada, must be considered in patients presenting with furuncles that do not respond to antibiotics, especially those with a central punctum. This is true even when the patient has not traveled outside of Canada and especially if there has been contact with livestock. Prompt diagnosis and treatment can prevent patient discomfort as well as reduce the risk of complications such as further invasion or secondary infection.
Competing interests
None declared.
This article has been peer reviewed.
References
1. Robbins K, Khachemoune A. Cutaneous myiasis: A review of the common types of myiasis. Int J Dermatol 2010;49:1092-1098.
2. Caissie R, Beaulieu F, Giroux M, et al. Cutaneous myiasis: Diagnosis, treatment and prevention. J Oral Maxillofac Surg 2008;66:560-568.
3. Solomon M, Lachish T, Schwartz E. Cutaneous myiasis. Curr Infect Dis Rep 2016;18:28.
4. Lagacé-Wiens PR, Dookeran R, Skinner S, et al. Human ophthalmomyiasis interna caused by Hypoderma tarandi, Northern Canada. Emerg Infect Dis 2008;14:64-66.
5. MacFadden DR, Waller B, Wizen G, Boggild AK. Imported and locally acquired human myiasis in Canada: A report of two cases. CMAJ 2015;187:22-25.
6. Slinger R, Scholten T. Facial furuncle on 3-year-old boy camping in Ontario. CMAJ 2003;168:1159.
7. McGraw TA, Turiansky GW. Cutaneous myiasis. J Am Acad Dermatol 2008;58:907-926.
8. Sanchez-Arroyo H. University of Florida, Entomology and Nematology. Featured creatures: Common cattle grub. Access-ed 27 January 2017. http://entnemdept.ufl.edu/creatures/livestock/cattle_grub.htm.
9. Fassler C, Lanco S, Denis A, et al. [Subcutaneous myiasis. A case report.] [Article in French.] Arch Pediatr 2000;7:840-843.
Ms Pharo, Mr Duivestein, and Ms McKeen are medical students at the University of British Columbia in the class of 2018. Dr Scaffidi Argentina is a UBC family medicine resident. Dr Marciniuk is a UBC pediatrics resident. Dr Bingham is a clinical instructor at UBC.

{kind=link}
{kind=link}
{kind=link}
{kind=link}