Beyond the cloudy lens: A physician’s guide to cataract treatment
Issue: BCMJ,
vol. 68, No. 6, July August 2026,
Pages 202-205 Review Articles
ABSTRACT: Cataracts are the progressive opacification of the crystalline lens. In British Columbia, cataracts are the leading cause of low vision, and their prevalence increases as the population ages. While most cataracts are age-related, additional risk factors include genetic predisposition; smoking; UVB exposure; corticosteroid use; diabetes; trauma; and prior ocular surgery, disease, or injury. Patients commonly present with progressive blurred vision, glare, and monocular diplopia. Diagnosis is typically made with slit-lamp examination, although reduced visual acuity and a diminished red reflex on ophthalmoscopy may raise suspicion. Cataract surgery is the only definitive treatment and is recommended when visual impairment significantly affects quality of life or interferes with ocular health management. Modern surgery involves phacoemulsification with intraocular lens implantation. It has excellent safety and efficacy profiles and is a cost-effective mechanism for restoring vision.
Cataracts are one of the most common causes of vision loss, but cataract surgery is extremely safe and is one of the most cost-effective treatments in medicine.
Cataracts are the progressive opacification of the transparent native crystalline lens. This eventually results in a decline in visual function for the patient and an obstructed view of the fundus during an ophthalmic exam. In British Columbia, cataracts are the most common cause of low vision, and their burden on British Columbians is expected to increase significantly in the coming years as the population’s average age increases.[1,2] The latest update to the BC Guideline for treatment of cataract in adults was published in 2021.[3] Most cataracts are age related: approximately 10% of the population has visually significant cataracts by age 60, 25% by age 70, and 50% by age 80.[1-3] Non-age-related risk factors that may accelerate or directly precipitate the formation of cataracts include genetic predisposition, smoking, UVB or other radiation exposure, prolonged corticosteroid use, uncontrolled diabetes, other systemic or ocular diseases, prior ocular surgery or trauma, and chemical or electrical injury.[3,4]
A cataract can be classified according to three types based on the location of the opacification: nuclear, cortical, or posterior subcapsular.[4] In most patients, more than one type exist simultaneously; however, the workup and treatment for any cataract type is the same.[3,4] While patient complaints may vary depending on the type and severity of the cataract, common complaints include worsening blurry vision, glare and halos from lights (especially when driving at night), colors becoming less vibrant, and monocular diplopia.[1-4]
Clinical assessment
Apart from occupational requirements (e.g., aircraft pilot, law enforcement) and/or legal requirements (e.g., driver’s licence renewal), there is no evidence to support the screening of cataracts in patients without visual complaints.[5,6] However, some patients may fail to notice their cataract progression or to verbalize a significant visual decline.[5,6] Thus, it is important for health care providers to recognize the risk factors and consider cataracts as a cause of functional decline. Visual impairment increases the risk of depression, withdrawal from social activities, avoidance of driving, and increased falls.[7,8] Patients may suddenly become aware of their cataract progression and present with a complaint of acute and rapid vision decline despite a subacute to chronic process.
The gold standard for assessing cataracts is with a slit lamp, but examination with an ophthalmoscope, combined with a Snellen visual acuity chart, can have a high positive predictive value.[5,6] A patient with cataracts may have a dull or absent red reflex and reduced visual acuity in the affected eye(s). When making the decision to refer a patient to an ophthalmologist for cataract assessment, one should specify the suspected eye(s), the functional impact of potential visual decline on the patient, and the patient’s interest in pursuing surgical treatment. While the only definitive treatment for cataracts is surgery, some patients may benefit from optimizing their refractive prescription, using tinted lenses or magnifying glasses as short-term solutions.[3-6]
Indications for cataract surgery
Once the patient is referred to an ophthalmologist for assessment, the decision to recommend surgery is made in a patient-centred process. The best corrected Snellen visual acuity is an important objective measurement, but subjective difficulties performing everyday activities such as driving, watching TV, or reading remain the deciding factor for most patients.[9] The presence of a cataract is not an indication for surgery, but having visually significant and quality-of-life-impairment is.[10] Another indication for cataract surgery in elderly patients is to improve cognitive function and slow dementia progression.[7,8,10] Finally, cataract surgery may be recommended if the lens itself is threatening ocular health or care.[10] Examples of such include secondary cataract-related glaucomatous disease (e.g., pupil block, acute angle closure) or impairment of visualization of the retina for the management of posterior segment disease (e.g., diabetic retinopathy, ocular tumors, age-related macular degeneration). It may also be recommended if driving criteria are not met.
In a presbyopic (age-related loss of ability to focus at near distances) patient who does not have visually significant cataracts or any of the above indications, an elective surgery known as “clear lens exchange” may be performed, although it is not covered by the BC Medical Services Plan (MSP).[11] This is identical to traditional cataract surgery, but its main goal is to reduce spectacle dependence in individuals who have not yet developed a cloudy lens but wish to improve their vision.[11] A patient who has undergone clear lens exchange in an eye will not develop a cataract in that eye in the future. Clear lens exchange, or cataract surgery, is distinct from laser refractive surgeries (LASIK or PRK), which alter the shape of the cornea without affecting the native lens.
Preoperative considerations
Surgical planning also requires physicians to screen for any health conditions that may compromise a safe operation. Common concerns include respiratory conditions that affect the patient’s ability to lie comfortably in the supine surgical position and psychiatric conditions that affect the patient’s ability to remain as stationary as possible.[12,13] While almost all cataract surgeries are performed with topical anesthesia with or without oral/intravenous sedation, a severely anxious patient or a patient suffering from dementia may require a retrobulbar block to achieve total orbital paresthesia and paresis.[13] General anesthesia may be indicated in most pediatric patients but very rarely in adults.[13]
In BC, almost all cataract surgeries are done unilaterally. However, when general anesthesia is required, patients may be considered for immediately sequential bilateral cataract surgery. This requires two sets of separately sterilized equipment, reprepping, and redraping the patient to minimize the risk of contaminated equipment affecting the eyes. With the exception of rare cases, immediately sequential bilateral cataract surgery is not the practice pattern in BC, although newer data suggest this approach may have benefits compared with unilateral surgery.[14]
Cataract surgery
Cataract surgery is typically performed in hospital operating rooms, day surgery units, or outpatient surgical centres. A typical surgery takes less than 20 minutes to perform. After dilation of the pupil in the preoperative area, the surgeon makes a small incision in the cornea and opens the capsule (“skin”) of the cataract, allowing an ultrasonic probe to access the cataract and fragment/aspirate it. After removal of the cataract lens, the artificial intraocular lens, usually made of acrylic, is placed in the capsular bag. Following surgery, patients are instructed to use antibiotic and anti-inflammatory eye drops for a number of weeks. Typically, each patient is followed up at 1 day, 1 to 2 weeks, and 4 to 6 weeks postoperatively, although follow-up intervals may vary between practitioners.
Intraocular lens options and refractive planning
Providing preoperative education when choosing artificial intraocular lenses and managing patient expectations according to their refractive goals play a large role in postoperative patient satisfaction.[15,16] A variety of artificial intraocular lenses are available for cataract surgery.[15-17] They may provide improved vision at a single point (monofocal) or for a range of vision (multifocal). Additionally, correction of astigmatism (imperfection in the curvature of the eye) can be achieved with toric artificial intraocular lenses, both monofocal and multifocal.[17]
MSP will pay for numerous monofocal artificial intraocular lenses. Patients who opt for monofocal artificial intraocular lenses generally choose to have a refractive goal of bilateral emmetropia, bilateral myopia, or monovision.[15-17] With bilateral emmetropia, the working distance is set to distance vision, and patients will have good distance vision but will rely on reading glasses for near vision.[15-17] A bilateral myopic target will leave the patient mildly nearsighted.[15-17] This will necessitate the use of glasses for distance vision but will maintain intact near vision.[15-17] Monovision is a combination of having one emmetropic eye and one myopic eye.[18] This strategy may provide increased spectacle independence at the cost of depth perception.[18]
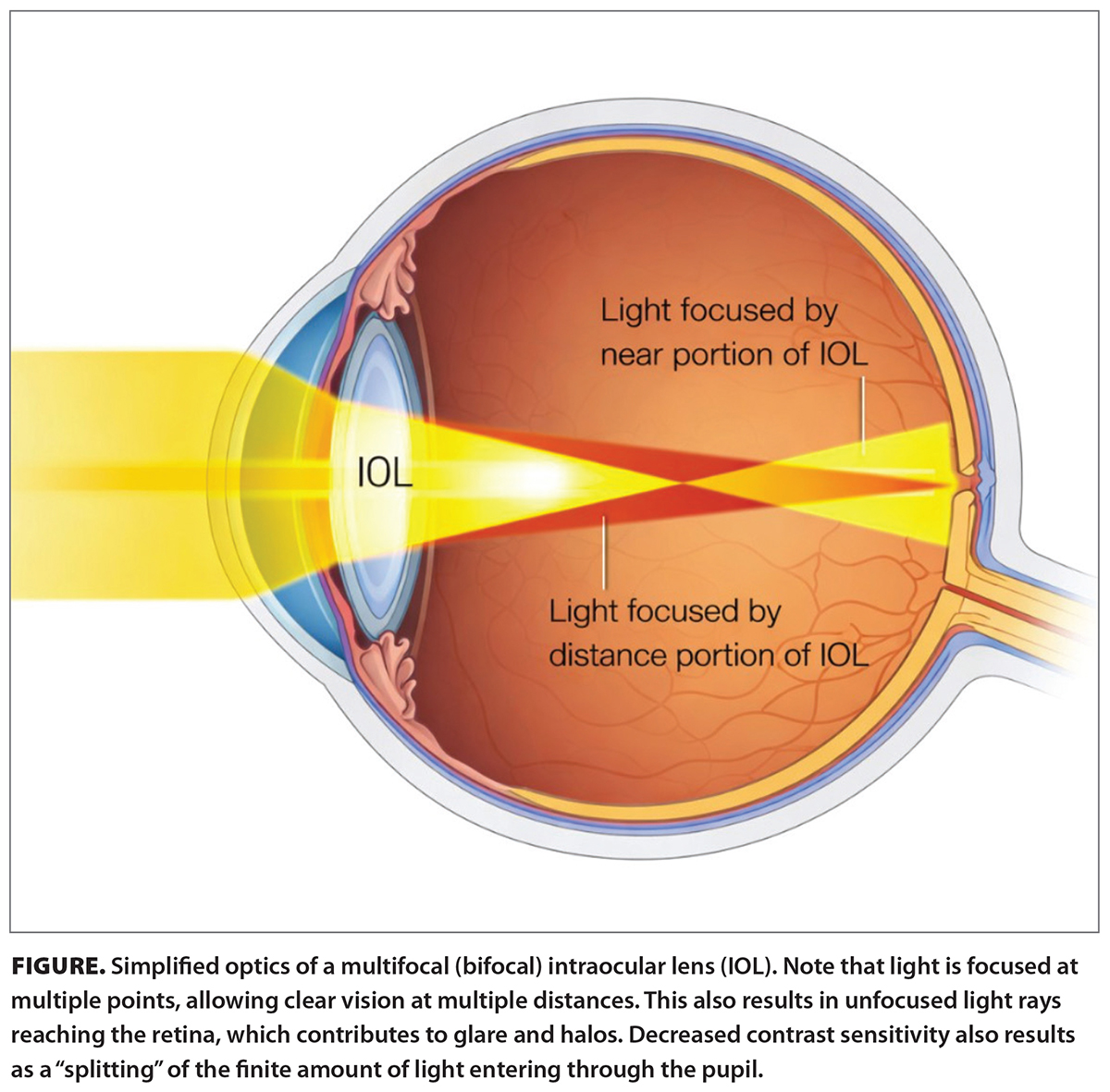 In patients with a strong desire for spectacle independence, alternative artificial intraocular lenses may be suitable options; they include multifocal artificial intraocular lenses [Figure], accommodative artificial intraocular lenses, and extended depth-of-focus artificial intraocular lenses.[19] These alternative artificial intraocular lenses are not covered by MSP; they are paid for by the patient to the hospital or health authority where the patient will have their surgery. Prices vary from less than $100 to more than $1600 per artificial intraocular lens, depending on the type selected. To optimize outcomes for these patients, surgeons typically require additional preoperative diagnostic testing, which is not covered by MSP. The main drawbacks of these lenses are increased risk of glare and halos and decreased light sensitivity (i.e., reduced contrast).[19] Patients who select these artificial intraocular lenses must be aware of potential challenges in low-light situations, such as night driving.[19] Finally, toric versions of each aforementioned artificial intraocular lens exist and can correct corneal astigmatism to further reduce spectacle dependence.[15-17,19] Toric artificial intraocular lenses necessitate placement in a specific axis; in less than 1% of cases, excessive rotational instability may necessitate a secondary repositioning surgery.[20]
In patients with a strong desire for spectacle independence, alternative artificial intraocular lenses may be suitable options; they include multifocal artificial intraocular lenses [Figure], accommodative artificial intraocular lenses, and extended depth-of-focus artificial intraocular lenses.[19] These alternative artificial intraocular lenses are not covered by MSP; they are paid for by the patient to the hospital or health authority where the patient will have their surgery. Prices vary from less than $100 to more than $1600 per artificial intraocular lens, depending on the type selected. To optimize outcomes for these patients, surgeons typically require additional preoperative diagnostic testing, which is not covered by MSP. The main drawbacks of these lenses are increased risk of glare and halos and decreased light sensitivity (i.e., reduced contrast).[19] Patients who select these artificial intraocular lenses must be aware of potential challenges in low-light situations, such as night driving.[19] Finally, toric versions of each aforementioned artificial intraocular lens exist and can correct corneal astigmatism to further reduce spectacle dependence.[15-17,19] Toric artificial intraocular lenses necessitate placement in a specific axis; in less than 1% of cases, excessive rotational instability may necessitate a secondary repositioning surgery.[20]
It is important to realize that the goal of cataract surgery is not complete spectacle independence. Rather, realistic expectations include a reduction in spectacle dependence, as well as visual improvement in tasks that had been prioritized before surgery. Last, artificial intraocular lens selection is a highly individualized process that considers patient lifestyle, patient desire for spectacle independence and tolerance for dysphotopsias, pre-existing eye conditions, and surgeon factors.
Outcomes of cataract surgery
Based on metrics such as quality-adjusted life-years and increased economic productivity, cataract surgery is one of the most cost-effective treatments in medicine.[21-23] More than 95% of patients obtain a satisfactory visual outcome in both the short term and long term.[22,23] Other benefits include a reduction in all-cause mortality, a reduction in falls leading to fractures, and a reduced fear of falling; increased independence in performing (instrumental) activities of daily living; and improved social connection, mental well-being, and cognitive function.[7,8,22,23] The most common risks of cataract surgery are dry eyes and posterior capsular opacification.[5,6,12]
Most postcataract patients develop posterior capsular opacifications and complain of a decline in vision.[6,12] This can easily be treated with a one-time, MSP-covered office laser procedure called YAG laser capsulotomy.[6,12] Another common postoperative complaint is dysphotopsia, which can present as positive or negative types.[12,23] Positive dysphotopsias present as light streaks, glare, starbursts, or light rings and occur in up to 67% of patients; negative dysphotopsias are described as a crescentic or linear shadow and occur in up to 27% of patients.[12,23] The etiology of dysphotopsias is attributed to patients adapting to “seeing” the edge of the intraocular lens, and almost all patients report spontaneous resolution of symptoms within the first year.[12,23] Another potential complication after cataract surgery is cystoid macular edema, a retinal swelling occurring in approximately 1% to 2% of patients.[12] The prognosis for postoperative cystoid macular edema is also good, with no further surgical interventions required to achieve a satisfactory visual outcome.[12]
Serious adverse events due to cataract surgery are rare but include endophthalmitis (infection), vitreous hemorrhage, retinal detachment, intraocular pressure spikes, and toxic anterior segment syndrome (severe noninfectious inflammation).[12] The cumulative incidence of sight-threatening complications postcataract surgery is less than 1%.[12] They are most likely to occur in the 2-week postoperative period, and patients should follow up with their surgeon immediately if they develop reduced vision, a worsening red eye, worsening eye pain, development of numerous floaters, and/or periorbital swelling.[12]
New technologies
Many innovative technologies have emerged in the world of cataract surgery. One of the most recent developments is femtosecond laser–assisted cataract surgery (FLACS).[24] In FLACS, a computer-guided laser performs multiple key steps that are usually performed manually by the surgeon.[24] While FLACS results in improved precision of each step compared with traditional manual techniques, there is no evidence that it has an improved safety profile or improved patient outcomes in the general population compared with standard cataract surgery.[24,25] The benefit of FLACS compared with traditional cataract surgery is supported by studies that have demonstrated that it can more predictably manage postoperative astigmatism and may improve outcomes in patients with select ocular comorbidities.[24,25] FLACS is considerably more expensive than standard cataract surgery and is not covered by MSP.
Another new technology is light-adjustable lenses. They are a type of artificial intraocular lens that allows vision to be fine-tuned in the weeks to months postcataract surgery using UV light.[26,27] This may lead to greater patient satisfaction and has proven to be safe, but again, it is an expensive option and is not covered by MSP.[26,27]
Conclusions
Cataract is an extremely common diagnosis that is most commonly associated with age. As the prevalence of cataracts continues to increase as the population in BC and Canada ages, it is important for all physicians to recognize the impact of this condition on patient lives. While cataracts cannot be prevented, onset can be delayed by advising smoking cessation, wearing sunglasses or hats for UVB protection, and managing diabetes.[3-6] Once cataract progression is detrimental to a patient’s quality of life, cataract surgery provides an extremely safe and cost-effective mechanism for restoring vision. Ongoing technological advancements within the realm of cataract surgery help ensure that patients’ independence, mental health, and even mortality rate are not negatively impacted by a cloudy lens.
Competing interests
None declared.
This article has been peer reviewed.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
References
1. Hashemi H, Pakzad R, Yekta A, et al. Global and regional prevalence of age-related cataract: A comprehensive systematic review and meta-analysis. Eye (Lond) 2020;34:1357-1370. https://doi.org/10.1038/s41433-020-0806-3.
2. Prokofyeva E, Wegener A, Zrenner E. Cataract prevalence and prevention in Europe: A literature review. Acta Ophthalmol 2013;91:395-405. https://doi.org/10.1111/j.1755-3768.2012.02444.x.
3. British Columbia Ministry of Health. Cataract – Treatment of adults. BC Guidelines. 26 May 2021. Accessed 1 May 2026. www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/cataract_guideline_final.pdf.
4. Delcourt C, Cristol JP, Tessier F, et al. Risk factors for cortical, nuclear, and posterior subcapsular cataracts: The POLA study. Am J Epidemiol 2000;151:497-504. https://doi.org/10.1093/oxfordjournals.aje.a010235.
5. Asbell PA, Dualan I, Mindel J, et al. Age-related cataract. Lancet 2005;365(9459):599-609. https://doi.org/10.1016/S0140-6736(05)17911-2.
6. Liu Y-C, Wilkins M, Kim T, et al. Cataracts. Lancet 2017;390(10094):600-612. https://doi.org/10.1016/S0140-6736(17)30544-5.
7. Evans JR, Fletcher AE, Wormald RPL. Depression and anxiety in visually impaired older people. Ophthalmology 2007;114:283-288. https://doi.org/10.1016/j.ophtha.2006.10.006.
8. van der Aa HPA, Comijs HC, Penninx BWJH, et al. Major depressive and anxiety disorders in visually impaired older adults. Invest Ophthalmol Vis Sci 2015;56:849-854. https://doi.org/10.1167/iovs.14-15848.
9. Desai P, Reidy A, Minassian DC, et al. Gains from cataract surgery: Visual function and quality of life. Br J Ophthalmol 1996;80:868-873. https://doi.org/10.1136/bjo.80.10.868.
10. Kessel L, Andresen J, Erngaard D, et al. Indication for cataract surgery. Do we have evidence of who will benefit from surgery? A systematic review and meta-analysis. Acta Ophthalmol 2016;94:10-20. https://doi.org/10.1111/aos.12758.
11. Alió JL, Grzybowski A, Romaniuk D. Refractive lens exchange in modern practice: When and when not to do it. Eye Vis (Lond) 2014;1:10. https://doi.org/10.1186/s40662-014-0010-2.
12. Chan E, Mahroo OAR, Spalton DJ. Complications of cataract surgery. Clin Exp Optom 2010;93:379-389. https://doi.org/10.1111/j.1444-0938.2010.00516.x.
13. Nouvellon E, Cuvillon P, Ripart J, Viel EJ. Anaesthesia for cataract surgery. Drugs Aging 2010;27:21-38. https://doi.org/10.2165/11318590-000000000-00000.
14. Lansingh VC, Eckert KA, Strauss G. Benefits and risks of immediately sequential bilateral cataract surgery: A literature review. Clin Exp Ophthalmol 2015;43:666-672. https://doi.org/10.1111/ceo.12527.
15. Nijkamp MD, Nuijts RM, Borne B, et al. Determinants of patient satisfaction after cataract surgery in 3 settings. J Cataract Refract Surg 2000;26:1379-1388. https://doi.org/10.1016/S0886-3350(00)00501-0.
16. Wasfi EI, Pai P, Abd-Elsayed AA. Patient satisfaction with cataract surgery. Int Arch Med 2008;1:22. https://doi.org/10.1186/1755-7682-1-22.
17. Lapp T, Wacker K, Heinz C, et al. Cataract surgery—Indications, techniques, and intraocular lens selection. Dtsch Arztebl Int 2023;120:377-386. https://doi.org/10.3238/arztebl.m2023.0028.
18. Wilkins MR, Allan BD, Rubin GS, et al. Randomized trial of multifocal intraocular lenses versus monovision after bilateral cataract surgery. Ophthalmology 2013;120:2449-2455.e1. https://doi.org/10.1016/j.ophtha.2013.07.048.
19. Gooi P, Ahmed IK. Review of presbyopic IOLs: Multifocal and accommodating IOLs. Int Ophthalmol Clin 2012;52:41-50. https://doi.org/10.1097/IIO.0b013e31824b87be.
20. Oshika T, Inamura M, Inoue Y, et al. Incidence and outcomes of repositioning surgery to correct misalignment of toric intraocular lenses. Ophthalmology 2018;125:31-35. https://doi.org/10.1016/j.ophtha.2017.07.004.
21. Brown GC, Brown MM, Menezes A, et al. Cataract surgery cost utility revisited in 2012: A new economic paradigm. Ophthalmology 2013;120:2367-2376. https://doi.org/10.1016/j.ophtha.2013.04.030.
22. Lansingh VC, Carter MJ, Martens M. Global cost-effectiveness of cataract surgery. Ophthalmology 2007;114:1670-1678. https://doi.org/10.1016/j.ophtha.2006.12.013.
23. Bournas P, Drazinos S, Kanellas D, et al. Dysphotopsia after cataract surgery: Comparison of four different intraocular lenses. Ophthalmologica 2007;221:378-383. https://doi.org/10.1159/000107496.
24. Donaldson KE, Braga-Mele R, Cabot F, et al. Femtosecond laser–assisted cataract surgery. J Cataract Refract Surg 2013;39:1753-1763. https://doi.org/10.1016/j.jcrs.2013.09.002.
25. Popovic M, Campos-Möller X, Schlenker MB, Ahmed IIK. Efficacy and safety of femtosecond laser-assisted cataract surgery compared with manual cataract surgery: A meta-analysis of 14 567 eyes. Ophthalmology 2016;123:2113-2126. https://doi.org/10.1016/j.ophtha.2016.07.005.
26. Schwartz DM. Light-adjustable lens. Trans Am Ophthalmol Soc 2003;101:417-436.
27. von Mohrenfels CW, Salgado J, Khoramnia R, et al. Clinical results with the light adjustable intraocular lens after cataract surgery. J Refract Surg 2010;26:314-320. https://doi.org/10.3928/1081597X-20090617-12.
Dr Yuan is a resident surgeon in the University of British Columbia Department of Ophthalmology. He completed his undergraduate studies and medical training at UBC. Prior to starting his residency, Dr Yuan completed a year-long glaucoma research fellowship at the University of Montreal. His research has been recognized with multiple awards for papers and presentations at international conferences, including most recently best paper and best oral presentation among residents and fellows at the American Society of Cataract and Refractive Surgery annual meeting. Dr Schendel is a clinical assistant professor at the UBC/Vancouver General Hospital Eye Care Centre. He received his MD at the University of Alberta and completed his residency training in ophthalmology at UBC. He completed a glaucoma fellowship at the Sydney Eye Hospital (University of Sydney, Australia). He teaches medical students, residents, and glaucoma fellows in his clinics, and his practice centres on surgical management of glaucoma and cataract. He is active in clinical research and administration and is president of the Canadian Glaucoma Society.
Excellent