The BC Rural Education Action Plan
Issue: BCMJ,
vol. 51 , No. 2 , March 2009 ,
Pages 73-76 Clinical Articles
The Joint Standing Committee on Rural Issues was established in 2000 as the result of negotiations between the British Columbia Medical Association and the Ministry of Health Services. The goal of the committee is to enhance the availability and stability of physician services in rural and remote areas of British Columbia by addressing some of the unique, demanding, and difficult circumstances faced by these physicians. The Rural Education Action Plan (REAP) is one of many initiatives implemented by the committee to address the medical human resource needs of rural BC through strategies that will attract, train, recruit, and retain medical trainees and professionals. Eligible students, residents, and physicians can benefit from REAP activities and funded strategies that allow them to advance their medical skills by serving in rural communities throughout BC.
The medical human resource needs of rural and remote areas in the province are being addressed through strategies that recruit and train medical professionals and encourage them to practise outside urban centres.
The Rural Education Action Plan (REAP) was established as a result of the Subsidiary Agreement for Physicians in Rural Practices, and is managed by the Joint Standing Committee on Rural Issues in collaboration with the UBC Faculty of Medicine, the Ministry of Health Services of British Columbia, and the British Columbia Medical Association. To address the medical human resource needs of rural BC, different strategies have been developed based on evidence that focused attention on education from high school through to undergraduate and postgraduate training and on into practice affects on recruitment for rural communities.[1-4] Evidence also supports admitting more students of rural origin to medical school.[5]
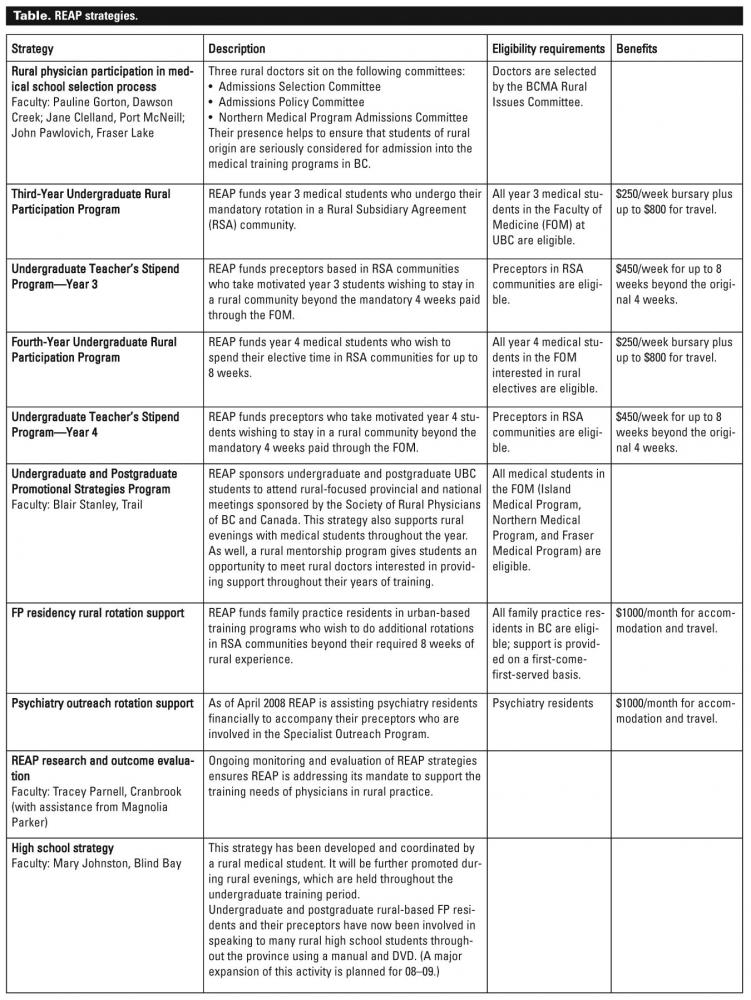
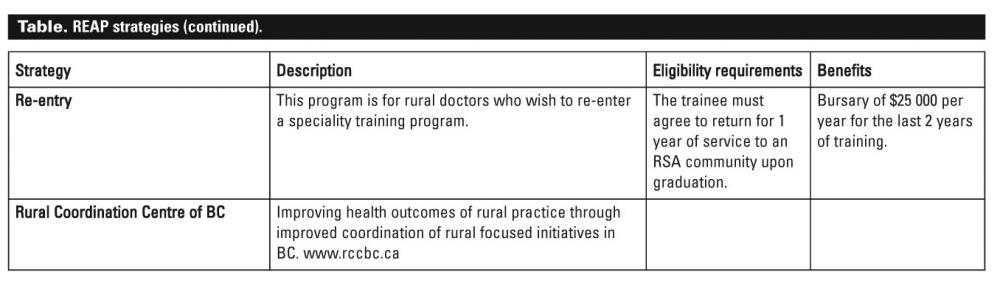
The Rural Education Action Plan began with a budget of $910 200 in 2001. As of April 2008 this budget had expanded to $3.1 million. The programs and initiatives supported by this money are summarized in the accompanying Table 1, Table 2, and Table 3.
{kind=link}
{kind=link}
In order to ensure that the objectives of REAP are attained efficiently and cost-effectively, a REAP faculty team was established. The team consists of physicians who are responsible for various strategies identified as effective in addressing the mandate. The program coordinator, Dr Whiteside, is responsible for monitoring and reporting on all REAP strategies. Dr Blair Stanley, a long-time practitioner in Trail, British Columbia, shares these responsibilities as the associate director.
Community liaison representatives
The community liaison representatives visit the 14 UBC postgraduate training sites around British Columbia in order to maintain communication between the academic centre and the communities. During these visits, they meet with faculty to discuss any possible teaching or administration issues. They also meet with and evaluate residents. This team consists of Dr Granger Avery, Port McNeill, Dr Marlowe Haskins, Smithers, and Dr Robb Sebastian, Grand Forks.
CME coordinator
The CME coordinator promotes and facilitates the delivery of rural continuing professional development (CPD) activities in collaboration with other provincial CPD initiatives. The coordinator also works along with the Society of Rural Physicians of Canada (BC) to arrange a conference in a rural community each year.
Undergraduate and postgraduate promotional strategies coordinator
Partial responsibilities of this position include accompanying approximately 30 medical students and 4 residents per year to separate Society of Rural Physicians of Canada conferences, one national and one provincial. The coordinator also speaks with medical students at rural evenings sponsored by the Family Medicine Interest Group.
Regional representatives
The regional representatives recruit and retain rural preceptors for undergraduate medical student rotations. This task has grown immensely over the past few years as UBC Medical School class size has expanded from 124 in 2001 to 256 in 2008.
Research and outcome evaluation faculty
The research and outcome evaluation faculty members determine which REAP strategies are most effective at recruiting and retaining rural physicians. This involves monitoring REAP strategies at undergraduate, postgraduate, and practice level.
Rural Subsidiary Agreement communities
More that 150 communities in BC have been designated as Rural Subsidiary Agreement (RSA) communities. Doctors in these smaller urban, rural, and remote areas of BC are eligible for funding. For more information please visit www.familymed.ubc.ca/__shared/assets/20080721AppendixB_RuralSubsidiaryAg....
Further information on REAP programs described here can be found at www.healthservices.gov.bc.ca/library/publications/year/misc/rural_progra.... The REAP coordinator can be reached at carl.whiteside@familymed.ubc.ca, Suite 300 – 5950 University Blvd., Vancouver, BC, V6T 1Z3, telephone 604 827-4188, fax 604 822-6950.
Rural Coordination Centre of BC
More information about REAP and other rural initiatives can be found at www.rccbc.ca, the web site of a virtual organization focusing on rural medical teaching and interprofessional training.
Competing interests
None declared.
References
1. Thistlethwaite JE, Shaw T, Kidd M, et al. Attracting Health Professionals into Primary Health Care: Strategies for Recruitment. Sydney: Australian Primary Health Care Research Institute, www.anu.edu.au/aphcri/Domain/Workforce/Thistlethwaite_25_FINAL.pdf (accessed 22 December 2008).
2. WONCA World Organisation of Family Doctors. Training for rural general practice. Report endorsed by the WONCA World Council Meeting, 9 June 1995. www.globalfamilydoctor.com/aboutWonca/working_groups/rural_training/trai... (accessed 22 December 2008).
3. Chan BTB, Degani N, Crichton T, et al. Factors influencing family physicians to enter rural practice: Does rural or urban background make a difference? Can Fam Physician 2005;51:1246-1247. www.cfpc.ca/cfp/2005/Sep/vol51-sep-research-5.asp (accessed 22 December 2008).
4. Society of Rural Physicians of Canada. Recruitment and retention: Consensus of the conference participants, Banff 1996. Can J Rural Med 1997;2:28-31. www.cma.ca/index.cfm/ci_id/37494/la_id/1.htm (accessed 22 December 2008).
5. James Rourke for the Task Force of the Society of Rural Physicians of Canada. Strategies to increase the enrolment of students of rural origin in medical school: Recommendations from the Society of Rural Physicians of Canada. CMAJ 2004;172:62-65. www.cmaj.ca/cgi/content/full/172/1/62 (accessed 22 December 2008)
Dr Whiteside is the coordinator of REAP and an assistant professor in the Department of Family Practice, Faculty of Medicine, University of British Columbia.