An assessment of British Columbia rural physicians’ continuing professional development needs
Issue: BCMJ,
vol. 51 , No. 6 , July August 2009 ,
Pages 250-255 Clinical Articles
Background: Previous studies have found that the educational needs of rural physicians differ from those of urban physicians. To characterize these differences in a Canadian context, a study was devised to assess the learning needs of British Columbia’s rural physicians and to develop an in-depth understanding of opportunities and challenges specific to their situation.
Methods: A multimethod research approach was employed. Two parallel surveys of BC rural GPs and specialists were completed and data were gathered from interviews and focus groups. The surveys included questions about clinical learning need areas, preferred continuing professional development (CPD) delivery methods, desired training on various educational technologies, attitudes toward current CPD offerings, and systemic strategies to enhance rural CPD opportunities. Results: Of the 1500 surveys distributed, 307 were completed by GPs and 141 were completed by specialists, for response rates of 31% and 28%, respectively. Physician-identified strategies to make CPD more relevant in a rural context were organized according to (1) clinical learning areas/preferred content, (2) preferred content delivery methods, and (3) strategies for support and coordination.
Conclusions: Findings from this study illustrate the unique educational needs of rural physicians while also highlighting the different needs of GPs compared with specialists. Results of this study also indicate how CPD providers might increase user satisfaction—insights that have helped with a new initiative, the Rural CPD Outreach Program.
Physicians seek hands-on, locally accessible, practical CPD taught by other rural physicians who understand the realities of rural practice.
While there is acceptance of the fact that rural physicians’ educational needs vary considerably from those of urban physicians, there is insufficient evidence to characterize these differences in the Canadian context, and particularly in British Columbia. Perceived challenges include:
• Geographical differences that affect access to educational activities.[1]
• Relevance of the educational content to rural physicians.[2-4]
• Opportunities for innovative approaches to educational programming.[5,6]
In this article the term “continuing professional development” (CPD) will be used in lieu of “continuing medical education.” Although the term “CME” has traditionally been used to describe ongoing professional education in medicine, many organizations are moving toward the term “continuing professional development” because it encompasses a broader range of relevant areas, such as practice management, interprofessional patient-centred care, and teaching in addition to clinical skills and evidence-based care. The term CPD also supports a wider variety of learning formats, such as small group and self-directed learning.
To develop an in-depth understanding of rural CPD needs, the authors invited rural physicians across BC to share their opinions and to outline the challenges they face. The insights obtained are, in many ways, reflective of the needs and challenges of rural physicians not only in BC, but also more generally in Canada and other countries. Applying these insights will allow CPD providers to improve rural physicians’ access to more effective educational programs.
The primary objectives of the study were to:
• Explore educational needs, including preferred content delivery methods, improvements in CPD coordination, and strategies to address unique CPD barriers.
• Determine what kind of support rural physicians require to actively engage in their own life-long learning, network with colleagues who have similar needs, and contribute to system improvements in CPD.
A steering committee was formed to guide survey design and to develop focus group and interview protocols. Members included representatives from various professional associations and governing bodies, government representatives, medical program directors, and rural physicians. The study aimed to determine the best way to offer CPD to rural physicians, given a paucity of regional data on the scope and content of their educational needs.
In July 2005 surveys were distributed—first by e-mail (with an online link to the survey form) and then by mail a week later—to potential participants identified through the British Columbia Medical Association database of physicians working within Rural Service Agreement communities.[7] The survey was designed to achieve a comprehensive understanding of rural CPD needs by capturing physicians’ preferences for CPD content, delivery methods, and attitudes toward access to rural CPD in general. Two parallel surveys were developed for GPs and specialists, with key sections including questions about:
• Clinical learning need areas.
• Preferred CPD delivery methods.
• Desired training on various educational technologies.
• Attitudes toward current CPD offerings.
• Systemic strategies to enhance rural CPD opportunities.
Ethics approval was obtained through the Behavioural Research Ethics Board at the University of British Columbia. Survey data were analyzed using SPSS software and qualitative data were analyzed for emergent themes.
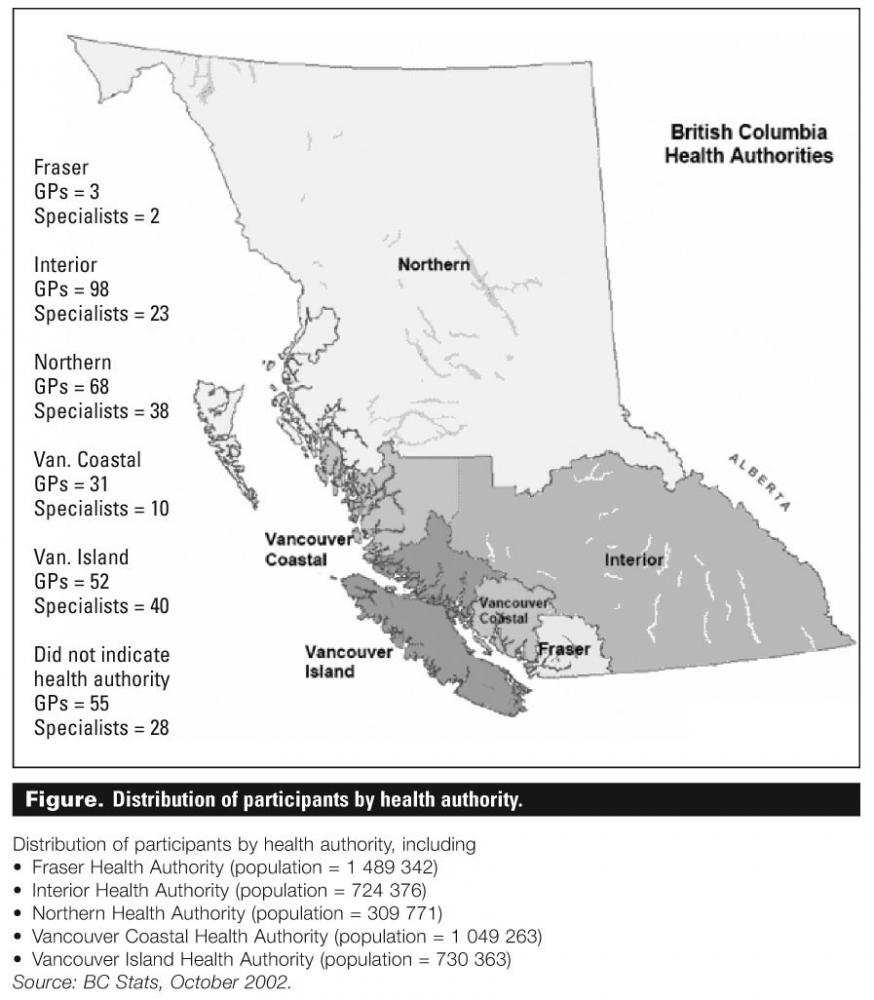
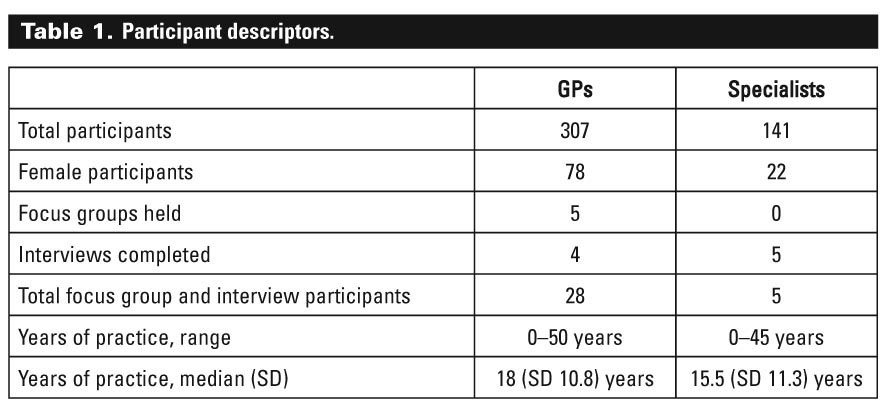
After 1500 surveys were distributed to rural practitioners throughout BC (see the Figure),[8] 307 GPs and 141 specialists (see Table 1) responded, for a response rate of 31% for GPs and 28% for specialists. Results were organized according to (1) clinical learning need areas/preferred CPD content, (2) preferred content delivery methods, and (3) strategies for support and coordination of rural CPD.
{kind=link}
{kind=link}
Preferred CPD content
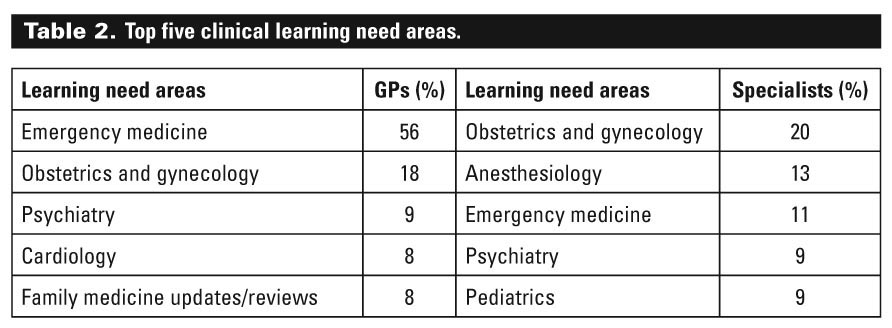
The top five clinical learning need areas preferred by GPs and specialists are shown in Table 2. Interprofessional education was also included in the survey as an area of exploration for CPD content. GP participants were “moderately” (30.2%) to “very interested” (12.3%) in increasing participation in interprofessional educational activities. Qualitative feedback elicited three main suggestions to improve the delivery of interprofessional CPD:
• Ensuring effective, local presenters.
• Offering better administration of the events at the regional level.
• Supporting structured, small-group learning sessions.
{kind=link}
Participants also commented that more interprofessional CPD would foster greater understanding of the challenges faced by colleagues in other disciplines, leading to more respectful relationships. In addition, participants felt interprofessional learning would increase CPD accessibility for all professional groups, especially at rural-focused conferences.
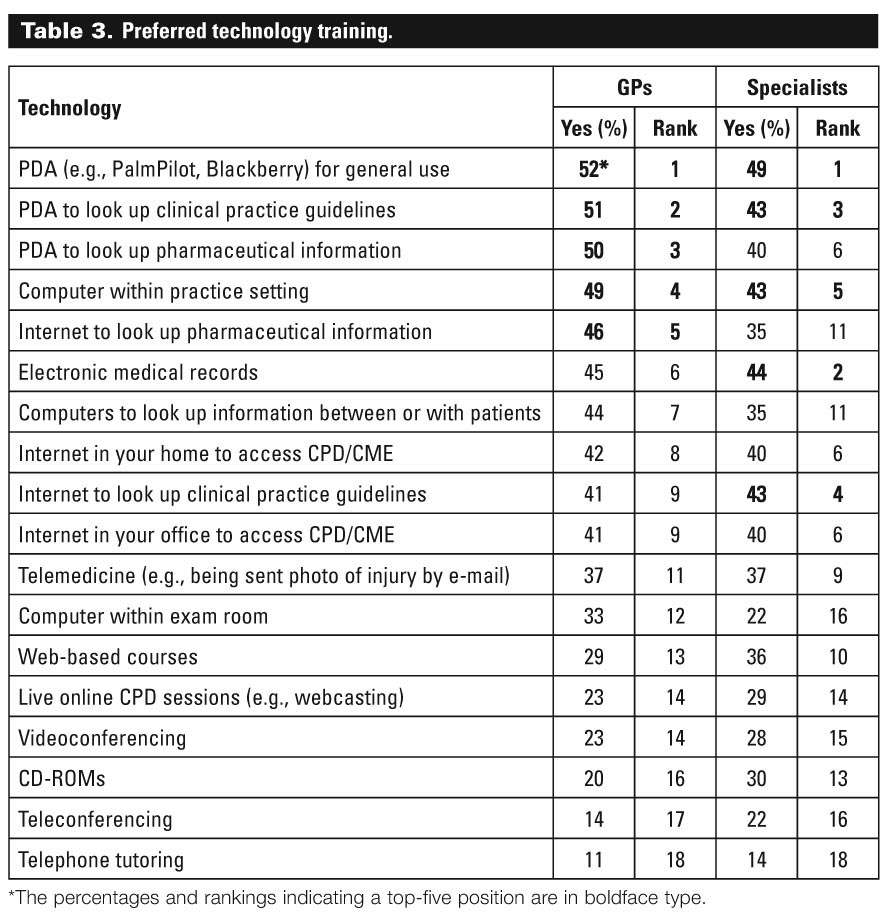
Finally, the survey asked about preferred technology training (see Table 3). Although both GPs and specialists ranked training in the general use of PDAs first, they did not agree on other preferences. For instance, specialists ranked training in the use of electronic medical records second while GPs ranked training in the use of this technology as a sixth preference.
{kind=link}
Preferred CPD content delivery methods
Both GPs and specialists indicated that professional isolation was a key challenge to CPD participation. Not surprisingly, the survey findings summarized in Table 4 show a greater preference for in-person CPD events.
{kind=link}
Strategies for support and coordination of rural CPD
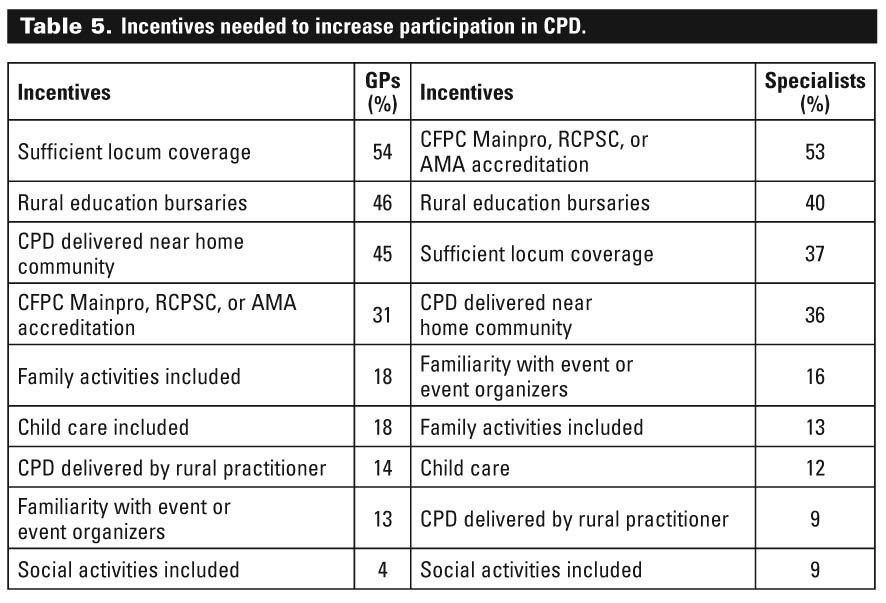
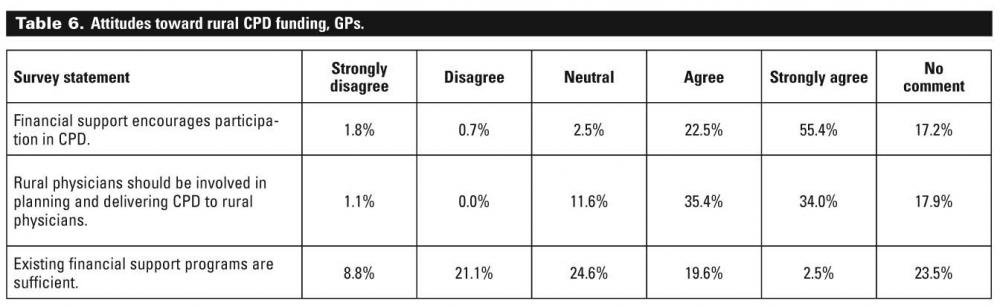
GPs and specialists had many suggestions for how CPD could be better supported to meet rural needs, including sufficient locum coverage and bursaries. The incentives physicians felt could increase participation in CPD activities are shown in Table 5. The attitudes of GPs and specialists regarding the funding of rural CPD are shown in Table 6 and Table 7.
{kind=link}
{kind=link}
{kind=link}
The study results suggest physicians seek hands-on, locally accessible, practical CPD taught by other rural physicians who understand realities of rural practice. Physicians also appreciate the opportunities provided by the CPD activities to maintain a support network with colleagues and mitigate against rural isolation. Both GPs and specialists rank attending conferences as their preferred method of learning.
Interprofessional teamwork is increasingly recognized as an essential aspect of health care reform. Indeed, the U.S. Institute of Medicine of the National Academies recommends that health care professionals develop and maintain proficiency in five core areas, one of which is working as part of interdisciplinary teams.[9] In the current study, physician participants viewed interprofessional education as a good setting for CPD learning, but only when it is locally based, oriented toward team learning, and tailored to meet the specific needs of all participants.
The Institute of Medicine also recommends using technology information as a core area for health professionals.[9] Topics of interest in technology training are diverse and range from PDA use and desktop computer activities to webcasting and telemedicine for service delivery. Generally, cost-effectiveness, ease of use, and integration into existing work patterns were highlighted as important factors for adoption of technology-enabled learning. Lack of basic computer skills remains a barrier, as does limited technological infrastructure in rural areas. Increasing the quality of audio/videoconferencing capabilities was identified as a key change required in improving rural CPD.
This study confirms results from a previous national study,[10] with congruent findings about clinical learning needs and preferred delivery formats. This study also extends previous national CPD research on physician needs to a more detailed level, showing differences in preference for delivery formats, barriers, incentives, and overall CPD attitudes within BC.[1] These findings support tailoring CPD topics to the localized needs of physicians and, ideally, having them delivered by local specialists.
The unique contribution of this study is in pinpointing specific, physician-identified strategies to support and coordinate rural CPD. For GPs, locum coverage is the best incentive to participate in CPD, while for specialists, attending accredited events, as opposed to nonaccredited, is the best incentive. The introduction of Revalidation in BC should further increase the interest in accredited events for rural physicians (see the College of Physicians and Surgeons of British Columbia web site for more information—www.cpsbc.ca/physicians-area/revalidation).
Strategies identified to make CPD offerings more relevant to rural practitioners support both centralized and regional solutions. Regional offerings of CPD serve to mitigate the problem of finding sufficient locum coverage and strengthen local GP-specialist relationships. However, participants also expressed a desire for a central body to coordinate the planning, development, and delivery of CPD events, to maintain an updated calendar of upcoming CPD events, and to facilitate reimbursement of available funds to support attendance.
A limitation of this study was the voluntary nature of the survey. Physicians who completed the survey were likely those engaged in CPD activities, while physicians not engaged in CPD were unlikely to have completed the survey, and the study may not have identified the needs of those physicians or others who have significant barriers to accessing CPD. Another limitation of the study involves interprofessional education. Since participants were all physicians, the survey did not capture the views of other professions, but simply reflects the opinions from the physician population toward interprofessional education.
Rural CPD Outreach Program
As a first step in more effectively engaging and addressing the CPD needs identified by this study, a central organizing body has been set up to tackle challenges faced by rural physicians. Based on the recommendations, suggestions, and data described here, and with support from the Rural Coordination Centre of BC, the Joint Standing Committee on Rural Issues approved funding for the UBC Division of Continuing Professional Development for a Rural CPD Outreach Program. Launched in October 2008, this program will work with and on behalf of rural physicians to build viable, practical, and effective rural CPD programming. Ongoing evaluation will determine if there is increased CPD engagement by rural physicians based on these targeted efforts, identify the changing needs of physicians over time, and enhance CPD offerings through a system of continuous quality improvement. To learn more about the Rural CPD Outreach Program, see page 263.
Competing interests
None declared.
References
1. Curran VR, Fleet L, Kirby F. Factors influencing rural health care professionals’ access to continuing professional education. Aust J Rural Health 2006;14:51-55. PubMed Abstract
2. Wilkinson D, Laven G, Pratt N, et al. Impact of undergraduate and postgraduate rural training, and medical school entry criteria on rural practice among Australian general practitioners: National study of 2414 doctors. Med Educ 2003;37:809-814. PubMed Abstract
3. Kelley ML, MacLean MJ. Interdisciplinary continuing education in a rural and remote area: The approach of the Northern Educational Centre for Aging and Health. Educ Gerontol 1997;23:631-649. Abstract
4. Delaney G, Lim SE, Sar L, et al. Challenges to rural medical education: A student perspective. Aust J Rural Health 2002;10:168-172. Abstract
5. Booth B, Lawrance R. Quality assurance and continuing education needs of rural and remote general practitioners: How are they changing? Aust J Rural Health 2001;9:265-274. PubMed Abstract
6. Zollo SA, Kienzle MG, Henshaw Z, et al. Tele-education in a telemedicine environment: Implications for rural health care and academic medical centers. J Med Syst 1999;23:107-122. PubMed Abstract
7. Joint Standing Committee on Rural Issues. Terms of reference. October 2005. www.health.gov.bc.ca/pcb/pdf/jsc_tor.pdf (accessed 12 May 2008).
8. BC Ministry of Health. Profiles of British Columbia’s six health authorities. www.bcbudget.gov.bc.ca/2007/sp/hlth/default.aspx?hash=10 (accessed 8 January 2009).
9. Institute of Medicine of the National Academies. Health professions education: A bridge to quality. 8 April 2003. www.iom.edu/CMS/3809/4634/5914.aspx (accessed 8 January 2009).
10. Curran VR, Keegan D, Parsons W, et al. A comparative analysis of the perceived continuing medical education needs of a cohort of rural and urban Canadian family physicians. Can J Rural Med 2007;12:161-166. Full Text
Dr Jarvis-Selinger is an assistant professor in the Department of Surgery at the University of British Columbia and associate director of the university’s eHealth Strategy Office. Ms Liman is the Aboriginal Portfolio research coordinator in the eHealth Strategy Office. Ms Stacy is the Language and Community Engagement Portfolio research coordinator in the eHealth Strategy Office. Dr Bluman is a clinical professor in the Department of Family Practice and assistant dean of the Division of Continuing Professional Development at UBC. Dr Ho is an associate professor in the Department of Surgery at UBC and director of the university’s eHealth Strategy Office. Ms Abizadeh is a researcher in the eHealth Strategy Office.