Anal cancer and human papillomavirus in HIV-positive men who have sex with men: A case report and review of the literature
Issue: BCMJ,
vol. 44 , No. 7 , September 2002 ,
Pages 374-378 Clinical Articles
This case study and literature review illustrate what is known about human papillomavirus-related anal squamous cell cancer in HIV-positive men who have sex with men, and describes which further epidemiological and medical investigations are warranted. Despite the rarity of anal cancer, its rate is disproportionately high in HIV-positive men who have sex with men. Anal cancer is associated with HPV, a common sexually transmitted disease, and HIV-positive men have a higher rate of HPV activity, relapse for anal warts, and high-grade dysplasia. As with screening for cervical cancer, an anal Papanicolaou test seems promising for this group, although more research is needed to determine the most effective screening and treatment methods.
Human papillomavirus (HPV), a common sexually transmitted disease that is almost universal in men infected with human immunodeficiency virus (HIV), is associated with the development of anal squamous cell carcinoma.[1-6] The incidence of anal squamous cell carcinoma in HIV-positive men who have sex with men doubles that of HIV-negative men who have sex with men.[2,7,8] Therefore, HIV-positive men who have sex with men who practise receptive anal intercourse are twice as likely to develop anal squamous cell carcinoma as HIV-negative men who have sex with men. Combination antiretroviral therapy does not prevent the development of anal cancer. However, antiretroviral use increases survival rate, and by living longer, HIV-infected men have a greater chance of developing anal squamous cell carcinoma.[2]
In this review, we report a case of an HIV-positive male patient who developed anal squamous cell carcinoma, and provide a brief review of the literature. Specifically, we report what is known about HPV-related anal squamous cell carcinoma in HIV-positive men who have sex with men, and which further epidemiological and medical investigations are warranted.
Like cervical cancer, anal cancer can be prevented through identification by screening. Are Pap smears the answer?
A 43-year-old man who has sex with men and who has advanced HIV disease, a CD4 count of 360 cells/µl, and a viral load of 3320 copies/ml presented with a 5-month history of anal pain and rectal discharge. The patient had a long history of anal symptoms, and initially thought his rectal bleeding was indicative of worsening hemorrhoids. The anal pain increased to the point where he sought medical attention for pain control.
Digital rectal examination identified a left-sided anal mass that occupied at least 75% of the circumference of his anal canal and was plastered against the left lobe of his prostate gland. There were multiple bilateral inguinal nodes, especially on the left side, where the largest node was 2 cm and tender.
He underwent a colonoscopy, and a 5 cm cauliflower-like, exophytic anorectal mass was noted. Biopsy confirmed a well-differentiated squamous cell carcinoma. Investigations for staging included magnetic resonance imaging and an endorectal ultrasound, which showed no evidence of vascular or lymphatic invasion. The final diagnosis was anal squamous cell carcinoma, clinical stage T3N3MO. Although testing was not done for HPV, this was the most likely cause.
His past medical history was noncontributory, except for HIV infection. He had been diagnosed with HIV 10 years previously, and his risk factors included having sex with men. His CD4 nadir was 90 cells/µl and he had been treated with multiple different antiretroviral regimens. He developed multidrug resistant HIV and started salvage therapy with eight antiretrovirals. He had no previous history of opportunistic infections or HIV-related malignancies.
The anal squamous cell carcinoma was treated with chemotherapy (5-FU) and radiation, which resulted in clinical improvement with tumor regression and resolution of palpable inguinal nodes. However, when therapy was completed, the anal squamous cell carcinoma relapsed, and he developed new-onset pneumaturia. A CT scan revealed an anovesicular fistula. He was treated symptomatically and referred for palliative care, including palliative chemotherapy (5-FU, cisplatin), and ongoing salvage antiretroviral therapy.
The incidence of anal squamous cell carcinoma in the United States is currently estimated at 0.8 per 100 000, one tenth that of cervical cancer, and is highest in sexually active adults aged 18 to 28 years old.[2,9] Even before the HIV epidemic, men who had sex with men had a higher incidence of anal squamous cell carcinoma (estimates range from 12.5 to 36.5 per 100 000) than the general population.[10]
The immune response appears to play a role in controlling HPV infection in the anal canal.[4] HIV-positive individuals with lower CD4 counts have compromised cell-mediated immunity and may be more prone to developing anal squamous cell carcinoma. Although HPV type 16 (which is oncogenic) is the most common genotype in both HIV-positive and HIV-negative men, HIV-positive men have a higher rate of HPV activity, relapse for anal warts, and high-grade dysplasia than do HIV-negative men.[11]
HPV transmission occurs through genital to genital, orogenital, and anogenital contact, and infrequently through hand to genital contact.[12] HPV can also be contracted through vertical and fomite (via inanimate objects such as sex toys) transmission.[13] Condoms do not prevent transmission since HPV may infect the base of the penis or the upper thigh, areas not covered by condoms.[1] The incubation period of HPV is usually 6 weeks to 8 months, but can be as long as several years. Most HPV infections are subclinical, and, hence, asymptomatic men may act as an HPV reservoir because the virus can live in a latent form in the urethra or prostate.[14]
In anal squamous cell carcinoma, rectal bleeding is the most common symptom and occurs in 45% of cases. Since bleeding is generally not profuse, and a mass is commonly palpated just above the anal sphincter, it is often mistakenly attributed to hemorrhoids.[12,15] The patient may present with other symptoms including pain or the sensation of a rectal mass (30%), tenesmus, pruritus, and bowel habit changes.[15] Twenty percent of patients present with no rectal symptoms.[12]
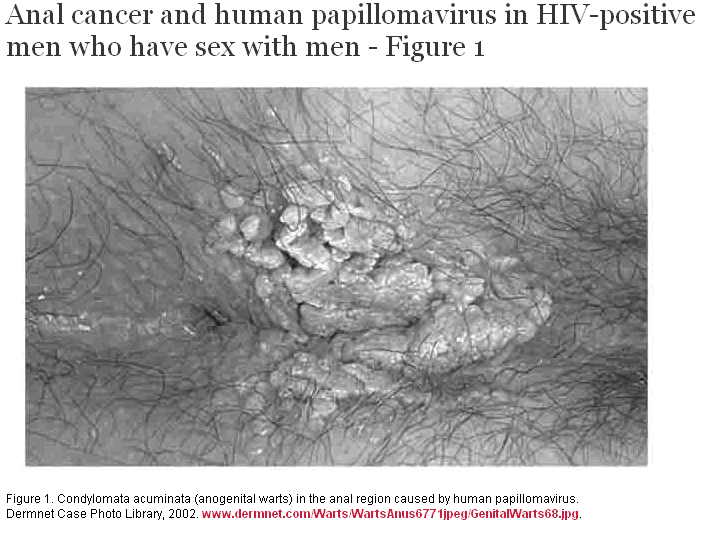
Visually detectable HPV infections may manifest as warts. A history of anal warts increases the risk of anal squamous cell carcinoma tenfold[16] and approximately 50% of patients with anal squamous cell carcinoma also have a history of anal warts.[12] HPV-induced warts (condylomata acuminata) look different from common skin disorders and cancers (Figure 1). Condylomata acuminata typically manifest as cauliflower-like masses, while lesions at risk for progression to carcinoma are commonly flatter. Warts that look atypical, for example, if they are pigmented, bleed, or are very large, should be biopsied to rule out anal squamous cell carcinoma. If there is palpable lymphadenopathy, aspiration or excisional biopsy of lymph nodes helps determine diagnosis and tumor staging.[15] Transrectal ultrasound may aid in determining tumor size and spread.[15]
{kind=link}
Screening for anal squamous cell carcinoma
Since the Papanicolaou (Pap) smear has successfully reduced the rate of cervical cancer by 90%, screening and treatment guidelines for anal lesions have followed the same diagnostic and management techniques used for cervical precancerous lesions.[1-7] Recommendations for individuals who practise receptive anal intercourse include annual anal Pap smears to test for HPV-related pathology. Recent analysis has projected that annual screening for HIV-positive men who have sex with men and biennial or triennial screening for HIV-negative men who have sex with men is cost-effective to prevent anal squamous cell carcinoma in these groups, and offers quality-adjusted life-expectancy benefits comparable to other clinical preventive measures.[1,10]
A screening program for anal squamous cell carcinoma has three components: history, physical, and laboratory. The history should include questions regarding anal bleeding, discharge, and pain. The physical examination consists of visual inspection of the perianal region for lesions as well as examination of the inguinal region for enlarged lymph nodes.[2] After visual inspection, to obtain a “male Pap” specimen, the patient should be in a knee/chest or lateral position. The anus is gently spread so that the anoderm pouts out, and a nonlubricated, moistened Dacron swab or cytobrush is inserted 2 cm to 3 cm. The swab or cytobrush is rotated 360 degrees, then removed and smeared onto a glass slide, which should then be sprayed with an ethanol fixation or, using the Thin-Prep method.[1,5,7] Lubrication should not be used when obtaining a specimen for cytology since it makes the slide more difficult to interpret. After cytology, a digital examination with lubrication should be performed to detect anal masses.[2]
Cytology specimens are classified in one of four ways: benign, atypical squamous cells of undetermined significance, low-grade squamous intraepithelial lesions, or high-grade squamous intraepithelial lesions.[7] Left untreated, some low-grade squamous intraepithelial lesions are thought to progress to high-grade squamous intraepithelial lesions, precursors to anal squamous cell carcinoma.[4] Figure 2 outlines the treatment algorithm for dysplastic lesions. If a dysplastic lesion is detected on cytology, the patient should be referred for high-resolution anoscopy, which utilizes acetic acid to examine the anal mucosa under a microscope. A colposcope, under magnification through the anoscope, can also be used to view the perianal skin, anal canal, and transition zone.[7] For areas that appear to be potential high-grade squamous intraepithelial lesions regions, biopsies, particularly at the squamocolumnar junction, should be performed. It is not yet clear if all moderate dysplasias should be treated. However, all individuals with high-grade squamous intraepithelial lesions, especially those with the most advanced forms, should be recommended for treatment.[2,7]
For high-grade squamous intraepithelial lesions, the recommended treatment is laser ablation or surgical excision. Pain from this procedure usually subsides within the first 7 to 10 days, and there are usually few complications. Patients with extensive circumferential lesions should not have their entire lesion removed in one surgical procedure due to the risk of complications such as anal stenosis. Options for these patients include sequential surgical procedures and/or close follow-up with biopsy of suspicious lesions. At this time, podophyllin, intralesional interferon, or other medical therapies for high-grade squamous intraepithelial lesions have not been proven to be effective. Small lesions might respond to local therapy applied in an office setting. These lesions may be treated with 80% trichloracetic acid, and require multiple applications over time for complete resolution, typically at intervals of 1 to 2 weeks.[2]
HIV-infected men have poorer treatment outcomes and shorter survival times than the general population.[16] In the general population, the majority of tumors are controlled locally with combined chemotherapy and radiation, and 5-year survival rates range from 65% to 85%.[8] Tumor size is an important prognostic factor; tumors 2 cm in diameter or less have a cure rate of 80%. Tumors 5 cm in diameter or larger are cured in less than 50% of cases.[12,15]
In HIV-negative individuals with anal squamous cell carcinoma, combined chemotherapy and radiation is the well-established standard treatment. Evidence indicates that HIV-positive patients, due to their decreased bone marrow reserves, tolerate chemotherapy less well than HIV-negative patients.[8] HIV-positive patients with CD4 lymphocyte counts of less than 200 cells/µl who receive more than 30 Gy of radiation tolerate treatment especially poorly.[12,15] Antiretroviral drugs also produce side effects that reduce treatment tolerability and may interact unfavorably with chemotherapy.[8]
Despite the potential drawbacks of combined chemotherapy and radiation, relatively healthy HIV-positive patients with anal squamous cell carcinoma should be treated with combined modality therapy. A reduction of radiation or chemotherapy is thought to compromise local control rates.[8] However, in severely immunocompromised individuals it may be more appropriate to use low doses of both radiation and chemotherapy.[15] Surgery is reserved as salvage treatment when residual tumor or local recurrence is detected.
Despite the rarity of anal cancer, the rate of anal squamous cell carcinoma is disproportionately high in HIV-positive men who have sex with men. As with cervical cancer, anal cancer may be prevented through identification by screening. HIV-infected men who have sex with men should be informed of anal cytology screening by their family physicians and at STD clinics. Screening is important to identify patients with high-grade squamous intraepithelial lesions and refer them for treatment. While preliminary results of Pap tests appear promising for this group, more research is warranted to determine the most effective screening treatment and methods.
References
1. Goldstone S. Anal dysplasia in men who have sex with men. AIDS Read 1999;9:204-208. Full Text
2. Palefsky JM. Anal squamous intraepithelial lesions in human immunodeficiency virus-positive men and women. Semin Oncol 2000;27:471-479. PubMed Abstract
3. Haga T, Kim S-H, Jensen RH, et al. Detection of genetic changes in anal intraepithelial neoplasia (AIN) of HIV-positive and HIV-negative men. J Acquir Immune Defic Syndr 2001;26:256-262. PubMed Abstract
4. Palefsky JM, Holly EA, Ralston ML, et al. Prevalence and risk factors for anal human papillomavirus infection in human immunodeficiency virus (HIV)-positive and high-risk HIV-negative women. J Infect Dis 2001;183:383-391. PubMed Abstract
5. Palefsky JM. Human papillomavirus-related tumors. AIDS 2000;14:S189-S195. PubMed Citation
6. Volberding P. Looking behind: Time for anal cancer screening. Am J Med 2000;108:674-675. PubMed Citation
7. Goldstone SE, Winkler B, Ufford LJ, et al. High prevalence of anal squamous intraepithelial lesions and squamous-cell carcinoma in men who have sex with men as seen in a surgical practice. Dis Colon Rectum 2001;44:690-698. PubMed Abstract
8. Cleator S, Fife K, Nelson M, et al. Treatment of HIV-associated invasive anal cancer with combined chemoradiation. Eur J Cancer 2000;36:754-758. PubMed Abstract
9. Pinto PA. Mellinger BC. HPV in the male patient. Urol Clin North Am 1999;26:797-807. PubMed Abstract
10. Goldie SJ, Kuntz KM, Weinstein MC, et al. The clinical effectiveness and cost-effectiveness of screening for anal squamous intraepithelia lesions in homosexual and bisexual HIV-positive men. JAMA 1999;281:1822-1829. PubMed Abstract
11. Sobhani I, Vuagnat A, Walker F, et al. Prevalence of high-grade dysplasia and cancer in the anal canal in human papillomavirus-infected individuals. Gastroenterology 2001;120:857-866. PubMed Abstract
12. Ryan DP, Compton CC, Mayer RJ. Carcinoma of anal canal. N Engl J Med 2000; 342:792-800. PubMed Abstract Full Text
13. Mayeaux EJ Jr, Spegener SD. Epidemiology of human papillomavirus infections. Hosp Pract (Off Ed) 1997;32:39-41. PubMed Citation
14. Frega A, Stentella P, Villani C, et al. Correlation between cervical intraepithelial neoplasia and human papillomavirus male infections: A longitudinal study. Eur J Gynaecol Oncol 1999;20:228-230. PubMed Abstract
15. Chawla AK, Willett CG. Squamous cell carcinoma of the anal canal and anal margin. Hematol Oncol Clin North Am 2001;15:321-344. PubMed Abstract
16. Bonnez W, Reichman RC. Papillomaviruses. In: Mandell D, Douglas R, Bennett J, et al. (eds). Principles and Practice of Infectious Diseases. 5th ed. Philadelphia, PA: Churchill Livingstone, Inc., 2000:1630-1644.
Elissa Press, BA, Gil Kimel MSc, Robert S. Hogg, PhD, Julio S.G. Montaner, MD, FRCP, and Natasha Press, MD, FRCPC
All authors are associated with the British Columbia Centre for Excellence in HIV/AIDS, St. Paul’s Hospital in Vancouver. Dr Hogg is also with the Department of Health Care and Epidemiology, University of British Columbia. Dr Montaner and Dr Press are also with the Department of Medicine at UBC.