By: Eris Nyx, BA [2] Jeremy Kalicum, MPH [3] Thomas Kerr, PhD [4]
A growing gap between paramedic and hospital overdose data in BC reveals that thousands of overdose cases go unclassified or unrecorded in emergency departments each year, obscuring the true impact of the toxic drug crisis and undermining effective public health response.
As the overdose crisis in North America continues unabated, data specific to overdose presentations in hospital remain critical to ongoing monitoring efforts and the evaluation and implementation of public policy. For example, a recent study in JAMA by Nguyen and colleagues, with the stated goal of assessing “the association of British Columbia’s adoption of the safer supply policy and subsequent decriminalization of drug possession with opioid overdose hospitalizations and deaths,” examined opioid-related hospitalizations using Canadian government counts of opioid overdose hospitalizations triaged with International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10-CA) codes T40.0–T40.4 and T40.6.[1] Although on the surface, such an examination would appear intrinsically robust, the true impact of drug-related overdoses on hospitals has likely been underreported due to gaps in surveillance and incomplete case classification within emergency departments. In fact, data from several sources indicate that many overdose cases are not fully classified during triage or may remain undocumented if patients leave against medical advice before triage. Such a surveillance gap would obscure the full scale of the overdose crisis and hamper the development of effective public health policy aimed at relieving strain on BC’s health care system. Bridging this gap will require better integration between paramedic services and hospital triage systems to ensure that overdose cases are accurately identified, categorized, and managed.
This surveillance discrepancy is evident when examining the following data sources:
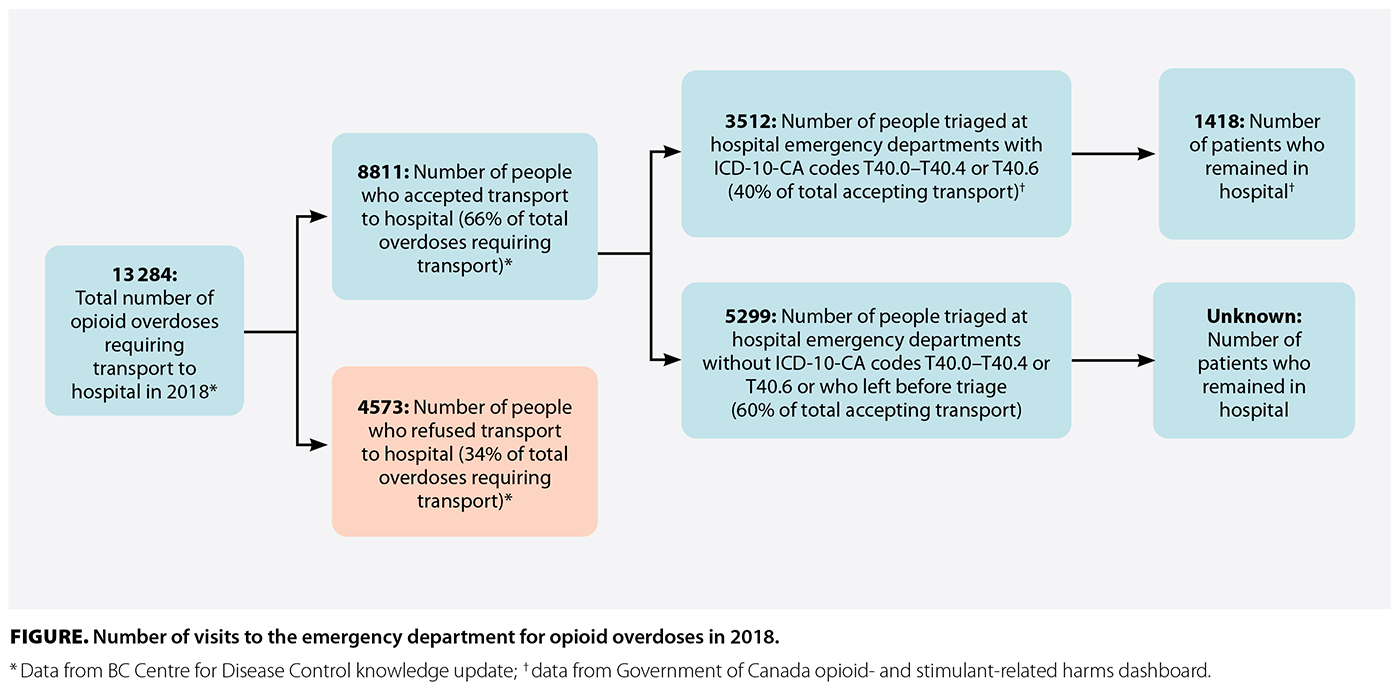
First, if we scrutinize the BCCDC’s 2019 knowledge update, we see a recorded 13 284 opioid overdoses requiring transport to hospital in 2018, 2 years after BC’s overdose emergency was declared.[4] The same document notes that while 8811 (66%) of these individuals were transported to hospital, 4573 (34%) were not.[4] During the same period, the Government of Canada reported 3512 opioid poisoning–related emergency department visits in BC, according to its opioid- and stimulant-related harms dashboard.[5] If the BCCDC data are accurate, the 3512 people counted by the Government of Canada represent only 40% of the 8811 people who should have arrived at the emergency department by ambulance because they overdosed. To rephrase, this discrepancy suggests that 5299 individuals who were taken to the emergency department to be treated for opioid overdose were transported to the emergency department but were not triaged with an opioid overdose code (i.e., ICD-10-CA codes T40.0–T40.4 or T40.6) or left the hospital before triage [Figure [13]].
 [13]
[13]
As this example illustrates, the lack of classification at emergency department triage and unclear surveillance around premature hospital discharge complicates the accurate surveillance of overdose cases. From the example, we can also see that a known 60% of transported overdose cases were not counted under an overdose ICD-10-CA code at triage, or people left against medical advice before they could receive a code. This means that only one-quarter of the total opioid overdoses requiring transport to hospital agreed to the transport, arrived, and were triaged at the emergency department with the correct ICD-10-CA code. Such a gap would distort surveillance data and obscure the full impact of the overdose crisis on the hospital system.
A key limitation of this analysis is the absence of recent provincial-level data linking overdose-related hospitalizations with paramedic transport. At present, the most recent publicly available data set containing linked and verifiable figures across BC Emergency Health Services and hospital systems dates to 2019. The reasons behind this lack of updated data remain unclear. This surveillance gap significantly hampers efforts to track emerging trends; evaluate the real-time impact of public health interventions such as safer supply and drug decriminalization; and make informed decisions regarding hospital system preparedness, resource allocation, and emergency response planning. Without timely, integrated data, the true burden of the toxic drug crisis on BC’s health care infrastructure remains obscured.
Beyond the absence of updated data, further discrepancies in overdose-related hospitalization figures may arise from clinical coding practices within emergency departments. Physicians frequently assign diagnostic codes based on a patient’s immediate clinical presentation or the condition currently being treated, rather than the underlying cause. For instance, a patient who overdosed might receive a diagnostic code for respiratory failure or cardiac arrest rather than an opioid-poisoning code. Such symptom-based coding can effectively hide overdose cases within hospital records, further contributing to systemic undercounting. While this approach aligns with standard clinical workflows, it underscores the urgent need for dual or bundled coding protocols that capture both presenting symptoms and the underlying overdose etiology to improve surveillance accuracy.
The failure to accurately capture overdose cases within hospital data has significant consequences. It diminishes the health care system’s ability to quantify demand, plan adequate staffing and emergency response capacity, and evaluate the effectiveness of critical interventions such as safer supply programs or expanded harm reduction services. When overdose cases are misclassified or omitted, public health strategies risk being underfunded, misdirected, or based on incomplete evidence. Addressing these issues through better integration of paramedic and hospital data systems, routine implementation of dual-coding practices, and mandated tracking of suspected overdose presentations should be understood not merely as a technical improvement but as an ethical imperative amid a public health emergency.
The low rates of accurate classification of overdose patients expose significant deficiencies in how overdose data are captured and, more broadly, handled in the health care system’s response to the toxic drug crisis. To mitigate these challenges, it is imperative to enhance data collection and refine classification systems, thus facilitating a meaningful response to this ongoing crisis.
This article was funded in part by the US National Institutes of Health (award no. U01DA038886).
None declared.
hidden
 [14] [14] |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License [14]. |
1. Nguyen HV, Mital S, Bugden S, McGinty EE. Safer opioid supply, subsequent drug decriminalization, and opioid overdoses. JAMA Health Forum 2025;6:e250101. https://doi.org/10.1001/jamahealthforum.2025.0101 [15].
2. Government of Canada. Opioid- and stimulant-related harms in Canada. Updated 13 September 2024. Accessed 5 November 2024. https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/ [16].
3. BC Centre for Disease Control. Unregulated drug poisoning emergency dashboard. Accessed 14 August 2024. www.bccdc.ca/health-professionals/data-reports/substance-use-harm-reduction-dashboard [17].
4. BC Centre for Disease Control. Topic: Declining transport to hospital for paramedic-attended overdose events [knowledge update]. 25 October 2019. Accessed 4 April 2024. https://web.archive.org/web/20211102152311/https:/www.bccdc.ca/resource-gallery/Documents/Statistics%20and%20Research/Statistics%20and%20Reports/Overdose/20191025_BCCDC%20Knowledge%20Update_Declining%20Transport%20to%20Hospital%20after%20non-fatal%20overdose%20event.pdf [18].
5. Government of Canada. Number of opioid-related poisoning ED visits in British Columbia, 2016 to 2023. 2024. Accessed 10 September 2024. https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/graphs.html?ind=377&unit=0 [19].
hidden
Ms Nyx is a master’s of science student in interdisciplinary studies at the University of British Columbia. Mr Kalicum holds a master’s of public health degree from the University of Victoria. Dr Kerr is a professor and head of the Division of Social Medicine at UBC. All authors have extensive experience working alongside people who use drugs in Vancouver’s Downtown Eastside.
Corresponding author: Ms Eris Nyx, email: erissassafrasnyx@gmail.com [20].
Links
[1] https://bcmj.org/cover/december-2025
[2] https://bcmj.org/author/eris-nyx-ba
[3] https://bcmj.org/author/jeremy-kalicum-mph
[4] https://bcmj.org/author/thomas-kerr-phd
[5] https://bcmj.org/node/11007
[6] https://bcmj.org/sites/default/files/BCMJ_Vol67_No10_premise-overdose.pdf
[7] https://bcmj.org/print/premise/overdose-and-british-columbia-s-hospital-system-have-we-miscounted
[8] https://bcmj.org/printmail/premise/overdose-and-british-columbia-s-hospital-system-have-we-miscounted
[9] http://www.facebook.com/share.php?u=https://bcmj.org/print/premise/overdose-and-british-columbia-s-hospital-system-have-we-miscounted
[10] https://twitter.com/intent/tweet?text=Overdose and British Columbia’s hospital system: Have we miscounted?&url=https://bcmj.org/print/premise/overdose-and-british-columbia-s-hospital-system-have-we-miscounted&via=BCMedicalJrnl&tw_p=tweetbutton
[11] https://www.linkedin.com/sharing/share-offsite/?url=https://bcmj.org/print/premise/overdose-and-british-columbia-s-hospital-system-have-we-miscounted
[12] https://bcmj.org/javascript%3A%3B
[13] https://bcmj.org/sites/default/files/BCMJ_Vol67_No10_premise-overdose_Figure.jpg
[14] http://creativecommons.org/licenses/by-nc-nd/4.0/
[15] https://doi.org/10.1001/jamahealthforum.2025.0101
[16] https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
[17] http://www.bccdc.ca/health-professionals/data-reports/substance-use-harm-reduction-dashboard
[18] https://web.archive.org/web/20211102152311/https:/www.bccdc.ca/resource-gallery/Documents/Statistics%20and%20Research/Statistics%20and%20Reports/Overdose/20191025_BCCDC%20Knowledge%20Update_Declining%20Transport%20to%20Hospital%20after%20non-fatal%20overdose%20event.pdf
[19] https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/graphs.html?ind=377&unit=0
[20] mailto:erissassafrasnyx@gmail.com
[21] https://bcmj.org/modal_forms/nojs/webform/176
[22] https://bcmj.org/%3Finline%3Dtrue%23citationpop