ABSTRACT
Background: Palliative care is not yet routinely integrated into surgical services in Canada, for a variety of complex reasons. We explore the understanding of modern palliative care among British Columbia general surgeons and its potential role for their patients.
Methods: Surgeons were invited to participate in semi-structured interviews. Thematic analyses were conducted via interpretive description in an iterative approach.
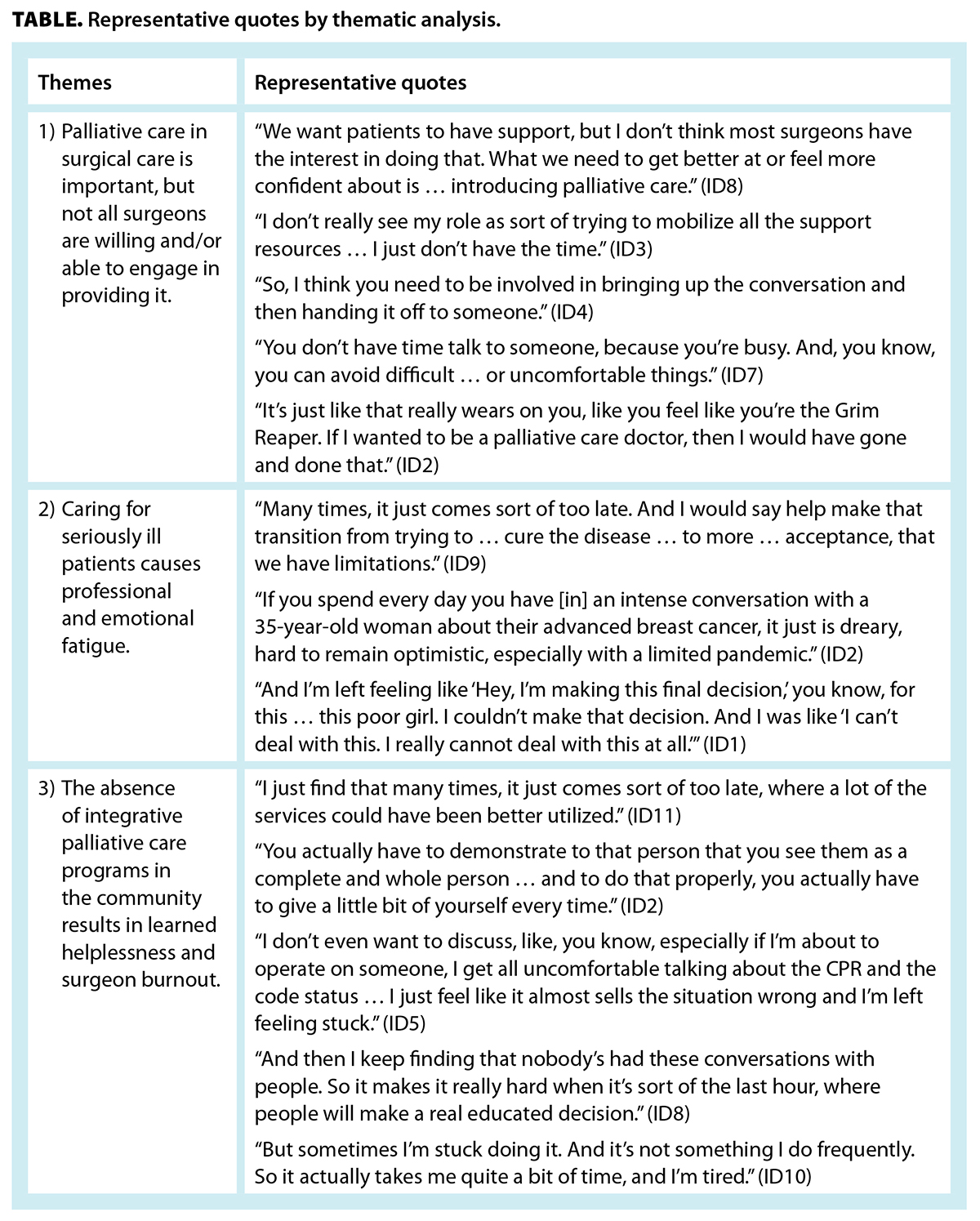
Results: Eleven interviews were conducted. Three overarching themes were identified: (1) palliative care in surgery is important, but not all surgeons are willing and/or able to engage in providing it; (2) caring for seriously ill patients causes professional and emotional fatigue; and (3) the absence of integrative palliative care programs in the community results in learned helplessness and surgeon burnout.
Conclusions: General surgeons’ concept of palliative care focuses on noncurative trajectories and represents a stagnant concept. Empathic, goal-concordant patient–physician conversations regarding surgical care paradigms are hindered by perceptions of resource limitations in a strained health care system.
Surgeons may be reluctant to provide palliative care for patients due to emotional and professional fatigue, lack of ability, and a lack of integrative palliative care programs.
The practices of general surgeons have traditionally been rooted in the imperative to relieve pain and suffering. However, as surgical innovations have grown in sophistication, palliation and cure have grown into diverging medical philosophies, and surgeons have not consistently explored basic palliative principles alongside active disease management, while not considering goals-of-care discussions until standard treatments are considered futile.[1-3] Physicians’ erroneous assumptions of patients’ goals drive prolonged and unwanted life-sustaining treatments at a high cost, both financially and morally.[1,2]
Shared decision making is a fundamental tenet of surgical care.[3-5] Despite robust evidence demonstrating significant benefits and improved patient outcomes from early and simultaneous integration of palliative care with disease-directed treatment,[5-7] there has been little uptake within the general surgical community.[8-10]
The palliative approach to care includes basic symptom management, good communication, and coordination of multidisciplinary care. It is a responsibility of all health care professionals. Where needs are complex, a specialist palliative care professional may be necessary, but they are in limited supply, particularly in rural and remote areas. Many patients also lack family doctors, which places pressure on specialist services’ capacity. Surgeons are therefore required to provide at least basic palliative care as a core competency.[11] They need to transparently discuss the probabilities of different outcomes and negotiate the challenges of achieving patient goals, in addition to juggling their workload. An increasing number of publications detail the impact of demands on Canadian physicians in a health care system crippled by limited resources and burgeoning documentation requirements, which is contributing to moral distress, burnout, and postpandemic fatigue.[12-14 [12]]
The research team consisted of clinicians at the University of British Columbia in general/surgical oncology (C.W.L.), surgical education/surgical oncology (R.C.), palliative care (P.H.), general surgery residency (K.M.T.), and undergraduate studies (J.Z.).
BC general surgeons were contacted via email in 2020 and invited to complete an anonymous computer-based survey that explored training, clinical experiences, and self-perceived competency in goals-of-care discussions and end-of-life care (data available from the corresponding author upon request). The survey was used to garner interest in and encourage thoughtful consideration of personal experiences of clinical palliative care and assess interest in participating in semi-structured interviews. The survey data did not inform interview responses because participants were de-identified, and the survey data do not correlate with interview data.
The interviewers (C.W.L., J.Z., and K.M.T.) asked open-ended questions related to exposure to palliative care as a surgical trainee, formal palliative care or enhanced communication skills training, specialist palliative care engagement, understanding of palliative care services as they apply to surgical patients, and current access to palliative care for patients.
Confidentiality was maintained by de-identifying interviewees prior to data analysis and reporting aggregate responses only. Interviews were audio- or video-recorded and were transcribed verbatim. All recordings were stored in password-encoded software available only to the study coordinators. Interviewee demographics were not collected to protect participant confidentiality and to be consistent with qualitative thematic analysis using interpretive description, as described by Thorne and colleagues.[15] This method emphasizes the generation of clinically relevant information through the interpretation of themes derived from the data rather than on demographic variables, in which the goal is to capture the richness and complexity of human experiences that transcend demographics.
The transcripts were manually reviewed for accuracy through line-by-line comparison with audio recordings and were analyzed via thematic analysis of interpretive description, as described by Thorne and colleagues.[15] We met virtually and in person on numerous occasions to discuss, review, and refine themes after each interview was conducted and upon completion of all interviews. The study included all participants who were available and willing to participate in interviews. In keeping with interpretive description thematic analysis, sample size is reflective not of generalizability but rather of the depth of relevance of the insights derived from patterns across participants.[15]
Ethics board approval was obtained from the BC Cancer Research Ethics Board in 2020.
Eleven semi-structured interviews were conducted with surgeons. Three distinct themes emerged:
See the Table [13] for surgeon quotes by theme.
 [13]
[13]
Participants echoed the importance of a palliative approach to care for patients with critical or life-limiting illness. There was unanimity on the need for palliative care services at the end of life, to transition into hospice, or when cure was unachievable. Surgeons rarely initiated discussions about including a palliative approach to care as part of treatment goals. Many surgeons believed palliative care equated to end-of-life care.
Surgeons described scenarios in which palliative care services were offered when no other treatment options seemed clinically reasonable. None of the participants described experiences in which palliative care services were introduced and integrated early during treatment. Many participants discussed experiences with patients in emergency scenarios who did not understand the severity and life-limiting nature of their disease prior to presentation to the emergency room, hence having no framework for the illness they were experiencing. In cases where patients were told what diseases they had, palliative care was rarely incorporated into their treatment plans unless disease-modifying treatment options were no longer deemed suitable. Participants shared experiences in which they felt reluctant to use the term palliative for fear of alienating patients or obliterating hope.
Due to a lack of awareness of the resources available within the hospital or immediate community, many surgeons rarely initiated discussions about the purpose, benefits, and rationale of palliative approaches to care, even when appropriate. “I don’t think most surgeons have the interest in doing that. What we need to get better at or feel more confident about is, like, introducing palliative care. So, we need to know what’s involved, but the breaking of bad news … do not shy away from that … we need to do better introducing people to die.” (ID8)
Participants were aware of their patients’ suffering. They shared stories about how patients felt dismissed by the health care system prior to developing acute illnesses and how some patients could have felt marginalized by the lack of care and continuity in their communities. Many surgeons expressed strong commitments to whole patient care but found it personally challenging due to a lack of time, unfamiliarity with referral processes, and a lack of awareness of community resources.
Implementing palliative care services was consistently viewed as needing to be provided only when surgery was no longer safely recommended or was considered futile. This notion was in keeping with the opinion that palliative approaches are mutually exclusive with active treatment. Unwillingness to engage in end-of-life conversations was also due to the sentiment of misplacement of responsibility onto the surgeon. Participants recalled these conversations as chaotic and emotionally charged, leaving fragments of guilt and distress after engaging in life-modifying conversations.
“And so you’ve tried everything. And that’s when you quit looking at the patient as a whole, and how they’re doing and what their goals there might be, looking at the broader picture… . These activities are really, incredibly invasive indicates a painful and possibly not effective intervention, [which] would be offering them the opportunity to talk to someone about quality of life rather than, you know, going full bore to the end, and then [we are] just exhausted … from what we’ve done to them.” (ID4)
While acknowledging the importance of using an integrated palliative approach to care, general surgeons did not express interest in additional learning opportunities to develop communication skills targeted at advance care planning and goals-of-care discussions. Many participants readily discussed the availability of specialist palliative care consultants in their hospitals but knew little about the community palliative care resources available. The principal reason for this was the conflicting demands of workload, but respondents also revealed that they referred late, if ever.
“When I’ve kind of maxed out where I feel comfortable going with medications, getting someone to … come and offer advice for that beyond just kind of the standard cocktail, you know, when you [start] having to adjust, I think there’s often been an inappropriate delay at our site. And in that … regard, just because, again, there’s not somebody dedicated to a palliative care service here.” (ID10)
Supplementary data are available from the corresponding author upon request.
General surgeons in this study expressed a genuine desire to provide whole patient care; however, they did not feel it was their responsibility. There was discomfort and a lack of knowledge about how to connect patients with community palliative care resources and reluctance to have goals-of-care conversations. Low comfort levels derive from multilayered negative personal and interprofessional experiences.[16] Our study revealed that most general surgeons said they were comfortable with their skills in discussing prognoses, death, and surgical outcomes; however, they had little interest and motivation in actually doing so. Surgeons conveyed strong notions of burden in engaging in quality-of-life discussions, adding that they were already overwhelmed by the demands of their existing practices and responsibilities.
Until recently, palliative care discussions were rarely taught in traditional surgical training.[17] Participants in this study expressed feeling distress, uncertainty, and frustration with the health care system regarding access to and support provided by palliative care services when needed. These conversations involved near-death or end-of-life situations. The rarity of these conversations perpetuates the misconception that palliative care is relevant only close to end of life, when it offers a holistic approach in the treatment and support of patients with serious illnesses from the time of diagnosis. Recognition of this outdated misperception is an opportunity for re-engagement and education.
Eliciting patient goals during emergencies in which there is no pre-existing therapeutic relationship between patient and surgeon can be particularly taxing. The best-case/worst-case framework for high-risk decision making offers a useful tool that can be applied in the emergency department or clinic.[18] Its success, however, depends on provider empathy, willingness to practise, and time spent building the surgeon–patient relationship. A recent systematic review of 18 studies on the outcomes of communication skills training among surgeons indicated that palliative care training interventions both objectively and subjectively improved surgeons’ confidence in communication, knowledge, and skills in symptom management.[18]
The “10 000-hour rule” of deliberate practice famously describes what many surgeons have learned over years of training: that it takes a lot of practice to be good at complex technical tasks.[19] To generate the same “muscle memory” with communication skills, the same degree of training and education should be considered for nontechnical skills. Surgical training programs across North America have adopted palliative care curricula since the early 2000s;[20,21] however, the implementation and success of these programs remains variable and limited.[22] Surveys of surgery residents revealed that although the level of clinical exposure to palliative care principles appeared adequate, many perceived that their education was not appropriately matched to their level and duration of training.[17,23] Continuing medical education on palliative care principles to support surgeons currently in practice is rare.[17] Mentorship and active role modeling have more impact than didactic teaching and have been shown to impart meaningful, practice-changing habits among trainees and junior staff.[24]
The surgeons we interviewed tended to focus on the deficits of the health care system. Workplace culture and regional disparities across the province negatively affected surgeons’ willingness to initiate early conversations with their patients. The overwhelming sentiment was that referral to a palliative care specialist was the most efficient and streamlined approach to care. The shortage of palliative care specialists and trained family doctors was perceived as a failing of the health care system rather than a missed opportunity to fill the gap as a member of the provider community. Surgeons wanted specialist colleagues and teams to be responsible for facilitating complex decision making and emphasized that engaging in emotionally laden goals-of-care discussions was not viewed as legitimate general surgery “work.” Disinterest was often linked to past experiences that involved deep feelings of stress, which subsequently resulted in depersonalization.
It is well established that stressors in the health care workplace contribute to dissatisfaction, burnout, attrition, and, in extreme scenarios, suicidal ideation.[24] Moral distress among surgeons exists on multiple levels, including individual, interpersonal, environmental, and community, as well as in policy.[25] Extrinsic protective factors were identified as having ethics training, early access to specialist palliative care support, more frequent discussions about goals of care, team collaboration, and colleague support.[25] When applied in appropriate and supportive scenarios, improved familiarity, training, and collegial support may alter a surgeon’s perception of their role and their abilities to conduct effective goals of care within their communities.[25]
Successfully navigating difficult conversations with surgical patients remains a responsibility of the surgeon. Although this study presents a unique reflection on a specific Canadian experience, the themes we identified are in keeping with the sentiments of surgeons globally regarding the consequences of limited health care resources. There is little disagreement that palliative approaches to care benefit surgical patients. Surgeons’ discomfort, unfamiliarity, and perception of inconvenience with goals-of-care discussions may be overcome by standardizing national training curricula that yield equivalent Royal College competency requirements in simple symptom management, with an emphasis on goals-of-care conversations, and in technical skills. Opportunities to guide changes in surgery practice paradigms include establishing workplace policies and advocacy programs that influence health policy to improve patient care, providing leadership by surgeon-led teams in collaborations and training programs, and creating formal mentorship models championed by surgeon advocates. Collectively, these efforts may facilitate the changes required by surgeons to adapt to evolving practice paradigms for improving overall patient care.
None declared.
The authors are grateful to Dr Kadhim Mustafa Taqi and Ms Jennifer Zhang for their considerable time and effort in data collection; without their efforts, this study would not have been possible.
This article has been peer reviewed.
 [14] [14] |
| This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License [14]. |
1. Berlin A, Carleton TJ. Concurrent palliative care for surgical patients. Surg Clin North Am 2019;99:823-831. https://doi.org/10.1016/j.suc.2019.06.001 [15].
2. Suwanabol PA, Reichstein AC, Suzer-Gurtekin ZT, et al. Surgeons’ perceived barriers to palliative and end-of-life care: A mixed methods study of a surgical society. J Palliat Med 2018;21:780-788. https://doi.org/10.1089/jpm.2017.0470 [16].
3. Dunn GP. Surgery, palliative care, and the American College of Surgeons. Ann Palliat Med 2015;4:5-9. https://doi.org/10.3978/j.issn.2224-5820.2015.01.03 [17].
4. Marterre B, Kopecky K, Miller P. Primary palliative care for surgeons: A narrative review and synthesis of core competencies. Ann Palliat Med 2022;11:885-906. https://doi.org/10.21037/apm-21-369 [18].
5. Brighton LJ, Bristowe K. Communication in palliative care: Talking about the end of life, before the end of life. Postgrad Med J 2016;92:466-470. https://doi.org/10.1136/postgradmedj-2015-133368 [19].
6. Zimmermann C, Swami N, Krzyzanowska M, et al. Early palliative care for patients with advanced cancer: A cluster-randomised controlled trial. Lancet 2014;383(9930):1721-1730. https://doi.org/10.1016/S0140-6736(13)62416-2 [20].
7. Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363:733-742. https://doi.org/10.1056/NEJMoa1000678 [21].
8. Hawley PH. The bow tie model of 21st century palliative care. J Pain Symptom Manage 2014;47:e2-e5. https://doi.org/10.1016/j.jpainsymman.2013.10.009 [22].
9. Cooper Z, Courtwright A, Karlage A, et al. Pitfalls in communication that lead to nonbeneficial emergency surgery in elderly patients with serious illness: Description of the problem and elements of a solution. Ann Surg 2014;260:949-957. https://doi.org/10.1097/SLA.0000000000000721 [23].
10. Schwarze ML, Redmann AJ, Alexander GC, Brasel KJ. Surgeons expect patients to buy-in to postoperative life support preoperatively: Results of a national survey. Crit Care Med 2013;41:1-8. https://doi.org/10.1097/CCM.0b013e31826a4650 [24].
11. Bernacki RE, Block SD. Communication about serious illness care goals: A review and synthesis of best practices. JAMA Intern Med 2014;174:1994-2003. https://doi.org/10.1001/jamainternmed.2014.5271 [25].
12. Ulrich CM, Grady C. Moral distress and moral strength among clinicians in health care systems: A call for research. NAM Perspect 2019;2019:10.31478/201919c.
13. Dodek PM, Cheung EO, Burns KEA, et al. Moral distress and other wellness measures in Canadian critical care physicians. Ann Am Thorac Soc 2021;18:1343-1351. https://doi.org/10.1513/AnnalsATS.202009-1118OC [26].
14. Webber J, Trothen TJ, Finlayson M, Norman KE. Moral distress experienced by community service providers of home health and social care in Ontario, Canada. Health Soc Care Community 2022;30:e1662-e1670. https://doi.org/10.1111/hsc.13592 [27].
15. Thorne S. Interpretive description. 1st ed. New York: Routledge; 2008. https://doi.org/10.4324/9781315426259 [28].
16. Ivey GD, Johnston FM. Barriers to equitable palliative care utilization among patients with cancer. Surg Oncol Clin N Am 2022;31:9-20. https://doi.org/10.1016/j.soc.2021.07.003 [29].
17. Bonanno AM, Kiraly LN, Siegel TR, et al. Surgical palliative care training in general surgery residency: An educational needs assessment. Am J Surg 2019;217:928-931. https://doi.org/10.1016/j.amjsurg.2019.01.008 [30].
18. Kruser JM, Taylor LJ, Campbell TC, et al. “Best case/worst case”: Training surgeons to use a novel communication tool for high-risk acute surgical problems. J Pain Symptom Manage 2017;53:711-719.e5. https://doi.org/10.1016/j.jpainsymman.2016.11.014 [31].
19. Zucker BE, Leandro L, Forbes K, et al. Training surgeons to optimize communication and symptom management in patients with life-limiting conditions: Systematic review. BJS Open 2023;7:zrad015. https://doi.org/10.1093/bjsopen/zrad015 [32].
20. Simon HA, Chase WG. Skill in chess: Experiments with chess-playing tasks and computer simulation of skilled performance throw light on some human perceptual and memory processes. Am Scientist 1973;61:394-403. https://iiif.library.cmu.edu/file/Simon_box00066_fld05052_bdl0001_doc0001/Simon_box00066_fld05052_bdl0001_doc0001.pdf [33].
21. Raoof M, O’Neill L, Neumayer L, et al. Prospective evaluation of surgical palliative care immersion training for general surgery residents. Am J Surg 2017;214:378-383. https://doi.org/10.1016/j.amjsurg.2016.11.032 [34].
22. Wancata LM, Hinshaw DB, Suwanabol PA. Palliative care and surgical training: Are we being trained to be unprepared? Ann Surg 2017;265:32-33. https://doi.org/10.1097/SLA.0000000000001779 [35].
23. Huffman JL. Educating surgeons for the new golden hours: Honing the skills of palliative care. Surg Clin North Am 2005;85:383-391. https://doi.org/10.1016/j.suc.2004.12.002 [36].
24. Han AY, Gentle CK, Stefanopoulos S, et al. Managing up: Approaching mentoring from a mentee’s perspective. J Surg Educ 2022;79:e161-e165. https://doi.org/10.1016/j.jsurg.2022.07.004 [37].
25. Millis MA, Vitous CA, Ferguson C, et al. To feel or not to feel: A scoping review and mixed-methods meta-synthesis of moral distress among surgeons. Ann Palliat Med 2023;12:376-389. https://doi.org/10.21037/apm-22-916 [38].
Dr Lee is a surgical oncologist with the Legacy Medical Group, Legacy Health Partners Hospitals, in Portland, Oregon. Dr Cheifetz is an associate professor at the University of British Columbia and medical lead of the BC Cancer Hereditary Cancer Program High Risk Clinic in Vancouver. Dr Hawley is a clinical professor and associate head of research in the Division of Palliative Care, Department of Medicine, UBC.
Corresponding author: Dr Christina W. Lee, chwlee@lhs.org [39].
Links
[1] https://bcmj.org/node/10878
[2] https://bcmj.org/author/christina-w-lee-md-frcsc-facs
[3] https://bcmj.org/author/rona-e-cheifetz-md-med-frcsc-facs
[4] https://bcmj.org/author/philippa-hawley-frcpc
[5] https://bcmj.org/sites/default/files/BCMJ_Vol67_No7_palliative-care.pdf
[6] https://bcmj.org/print/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care
[7] https://bcmj.org/printmail/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care
[8] http://www.facebook.com/share.php?u=https://bcmj.org/print/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care
[9] https://twitter.com/intent/tweet?text=Goal-concordant surgical care for patients: General surgeons’ experiences of palliative care&url=https://bcmj.org/print/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care&via=BCMedicalJrnl&tw_p=tweetbutton
[10] https://www.linkedin.com/sharing/share-offsite/?url=https://bcmj.org/print/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care
[11] https://bcmj.org/javascript%3A%3B
[12] http://12
[13] https://bcmj.org/sites/default/files/BCMJ_Vol67_No7_palliative-care_Table.jpg
[14] http://creativecommons.org/licenses/by-nc-nd/4.0/
[15] https://doi.org/10.1016/j.suc.2019.06.001
[16] https://doi.org/10.1089/jpm.2017.0470
[17] https://doi.org/10.3978/j.issn.2224-5820.2015.01.03
[18] https://doi.org/10.21037/apm-21-369
[19] https://doi.org/10.1136/postgradmedj-2015-133368
[20] https://doi.org/10.1016/S0140-6736(13)62416-2
[21] https://doi.org/10.1056/NEJMoa1000678
[22] https://doi.org/10.1016/j.jpainsymman.2013.10.009
[23] https://doi.org/10.1097/SLA.0000000000000721
[24] https://doi.org/10.1097/CCM.0b013e31826a4650
[25] https://doi.org/10.1001/jamainternmed.2014.5271
[26] https://doi.org/10.1513/AnnalsATS.202009-1118OC
[27] https://doi.org/10.1111/hsc.13592
[28] https://doi.org/10.4324/9781315426259
[29] https://doi.org/10.1016/j.soc.2021.07.003
[30] https://doi.org/10.1016/j.amjsurg.2019.01.008
[31] https://doi.org/10.1016/j.jpainsymman.2016.11.014
[32] https://doi.org/10.1093/bjsopen/zrad015
[33] https://iiif.library.cmu.edu/file/Simon_box00066_fld05052_bdl0001_doc0001/Simon_box00066_fld05052_bdl0001_doc0001.pdf
[34] https://doi.org/10.1016/j.amjsurg.2016.11.032
[35] https://doi.org/10.1097/SLA.0000000000001779
[36] https://doi.org/10.1016/j.suc.2004.12.002
[37] https://doi.org/10.1016/j.jsurg.2022.07.004
[38] https://doi.org/10.21037/apm-22-916
[39] mailto:chwlee@lhs.org
[40] https://bcmj.org/modal_forms/nojs/webform/176?arturl=/articles/goal-concordant-surgical-care-patients-general-surgeons-experiences-palliative-care&nodeid=67
[41] https://bcmj.org/%3Finline%3Dtrue%23citationpop